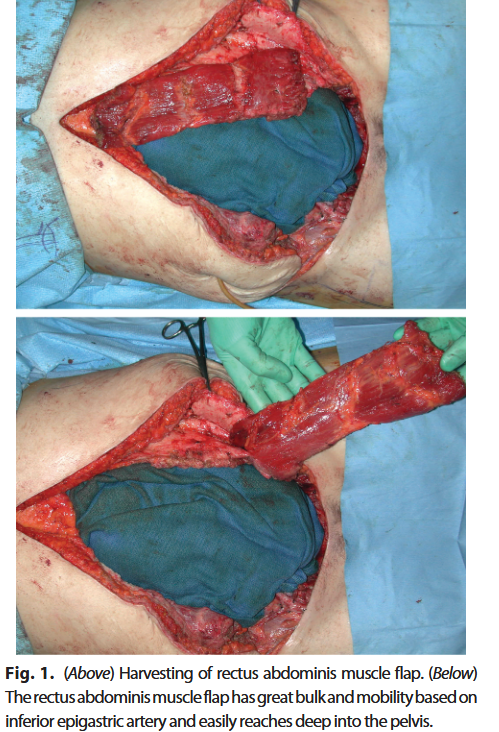
“Gynecologic malignancies are often treated with surgical resection and pelvic irradiation. The small bowel is most important in determining the dose of pelvic radiation because of its sensitivity to the effects of radiation. Enterovaginal fistulas in an irradiated field are rare and very challenging problems, often with devastating clinical and personal consequences. We investigated the use of the rectus abdominis muscle flap for the definitive treatment of recurrent enterovaginal fistula in the irradiated field. The rectus abdominis muscle has
ideal features for this use, including a long vascular pedicle, good bulk, low flap-related complication rates, and excellent graft survival.”