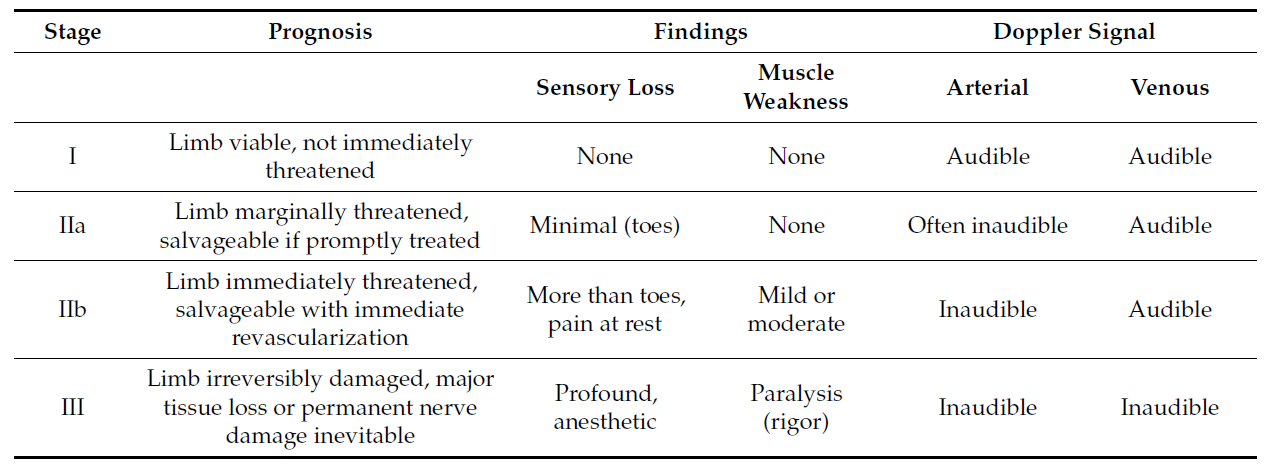
Rutherford classification for acute limb ischemia
Reply

Shackford SR. (2018). Venous Disease. In: Abernathy’s Surgical Secrets, 7th ed.: p. 357.
What is the difference between phlegmasia alba dolens and phlegmasia cerulea dolens?
“These two entities occur following iliofemoral venous thrombosis, 75% of which occur on the left side presumably because of compression of the left common iliac vein by the overlying right common iliac artery (May-Thurner syndrome). Iliofemoral venous thrombosis is characterized by unilateral pain and edema of an entire lower extremity, discoloration, and groin tenderness. In phlegmasia alba dolens (literally, painful white swelling), the leg becomes pale. Arterial pulses remain normal. Progressive thrombosis may occur with propagation proximally or distally and into neighboring tributaries. The entire leg becomes both edematous and mottled or cyanotic. This stage is called phlegmasia cerulea dolens (literally, painful purple swelling). When venous outflow is seriously impeded, arterial inflow may be reduced secondarily by as much as 30%. Limb loss is a serious concern and aggressive management (i.e., venous thrombectomy, catheter-directed lytic therapy, or both) is necessary.”
Chinsakchai K, et al. Trends in management of phlegmasia cerulea dolens. Vasc Endovascular Surg. 2011 Jan;45(1):5-14. Full-text for Emory users.

Bradbury AW, Adam DJ, Bell J, et al.; BASIL trial Participants. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: An intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplasty-first revascularization strategy. J Vasc Surg. 2010 May;51(5 Suppl):5S-17S.
Summary of BASIL trial recommendations: The BASIL trial suggests that those SLI patients who are likely to live ≥2 years are probably better served by a BSX-first strategy, preferably with vein. [37] Those SLI patients who are unlikely to live 2 years, and possibly those in whom vein is not available for bypass, are probably better served by a BAP-first strategy because they are unlikely to survive to reap the longer-term benefits of surgery, they may be more likely to suffer surgical morbidity and mortality, and because angioplasty is significantly less expensive than surgery in the short-term.
