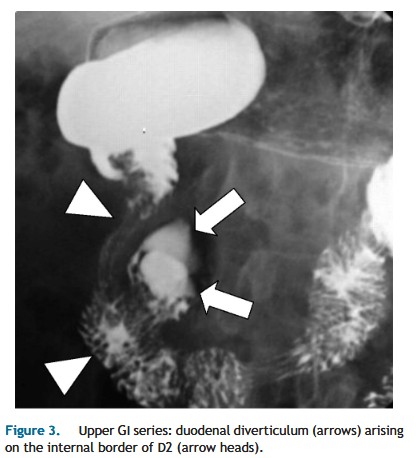
“Despite their frequent occurrence, DD are asymptomatic in 95% of cases, while 1 to 5% eventually become symptomatic. Intervention is indicated only for symptomatic duodenal diverticula(DD). Complications related to DD are rare but may be very severe; they include biliary or pancreatic obstruction, duodenal obstruction, perforation, or hemorrhage.
Endoscopic treatment is usually the first-line approach to biliopancreatic complications related to juxtapapillary DD and also for hemorrhagic complications. Indirect surgical
treatments include bilio-enteric bypasses and even duodenal exclusion. Direct surgical treatment consists of duodenal diverticulectomy, which has significant morbidity and mortality; prophylactic excision of asymptomatic DD is therefore not recommended.”