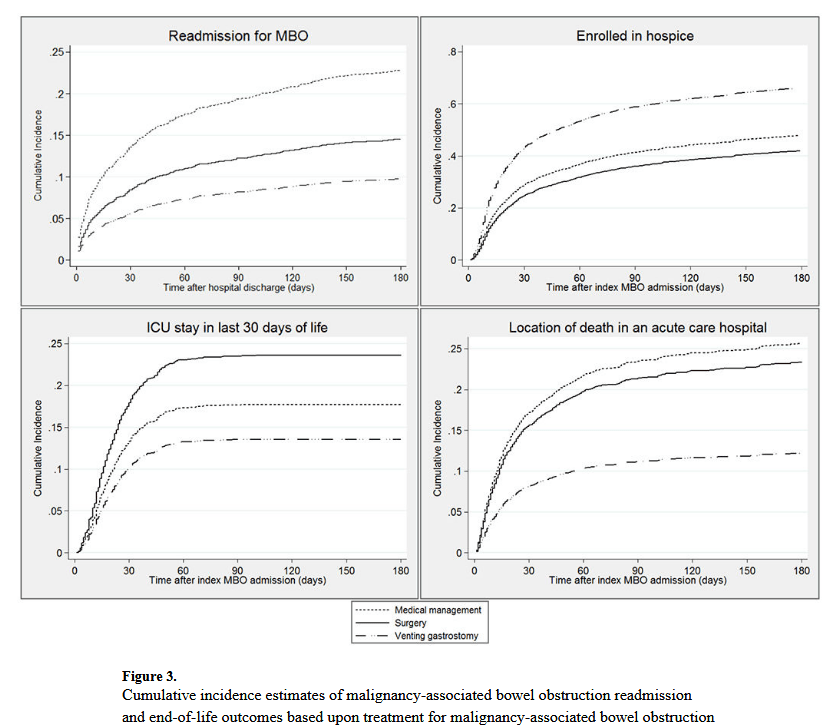
“Among patients with cancer, the estimated prevalence of malignancy-associated bowel obstruction (MBO) is 3-15%, including up to 51% in ovarian cancer and up to 28% in cancers of the gastrointestinal tract. MBO is among the most common palliative indications for surgical consultation5 and typically signifies a poor prognosis, with mean survival of 3-8 months in surgical cases and 4-5 weeks in those with inoperable MBO. Managing the considerable symptom burden associated with MBO frequently requires hospitalization and contributes to high-intensity healthcare utilization.1, In light of national efforts to address the poor quality and high cost of care near the end of life, it is critical to understand the relationship between treatment for complications of terminal cancer, such as MBO, and end-of-life (EOL) care.”
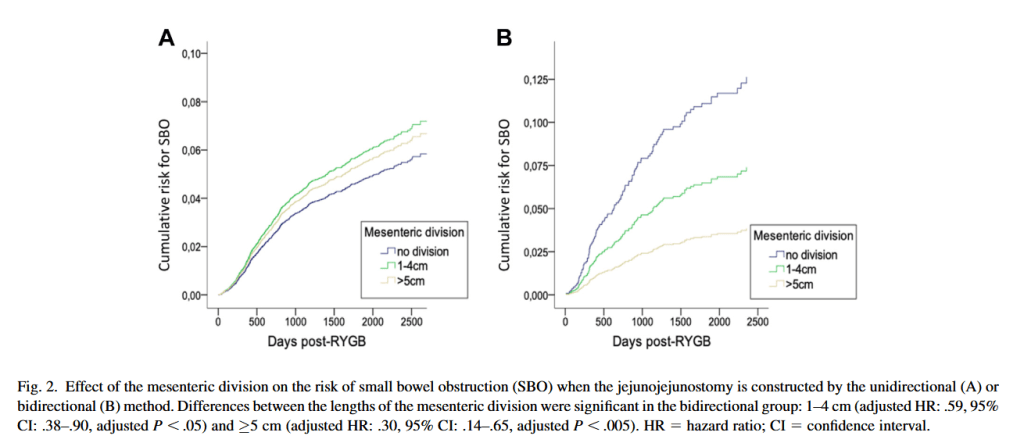
“Laparoscopic Roux-en-Y gastric bypass (RYGB) surgery is an effective bariatric procedure with excellent outcomes in terms of weight loss and reducing co-morbidities. Large series have demonstrated that the procedure can be performed with low postoperative morbidity and very low mortality. However, concerns have been raised about long-term complications, especially small bowel obstruction (SBO). In Sweden, RYGB is almost exclusively performed laparoscopically using the antecolic, antegastric Gothenburg technique. Since the technique was first described, alterations have been introduced to reduce the risk of internal herniation, but these modifications have been reported to increase the risk of kinking of the jejunojejunostomy (JJ). Our group has previously demonstrated that diagnostic laparoscopy in RYGB patients suffering from postprandial symptoms often reveals surgically correctable dysfunction/kinking at the JJ.”
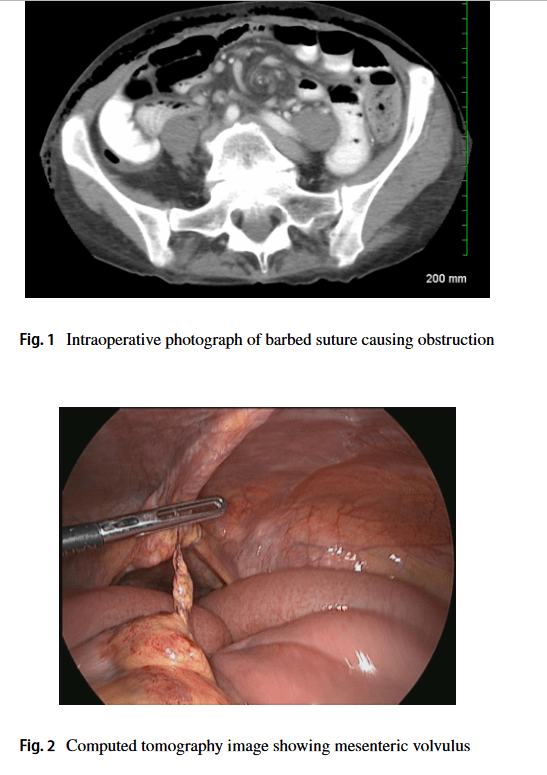
“Barbed suture has been adopted across all surgical specialties. One of the infrequent complications seen with the use of barbed suture is small bowel obstructions (SBOs). In this study, we perform a review of the literature and the Manufacturer and User Facility Device Experience Database (MAUDE) to characterize SBOs after the use of barbed sutures in a variety of operative procedures.”
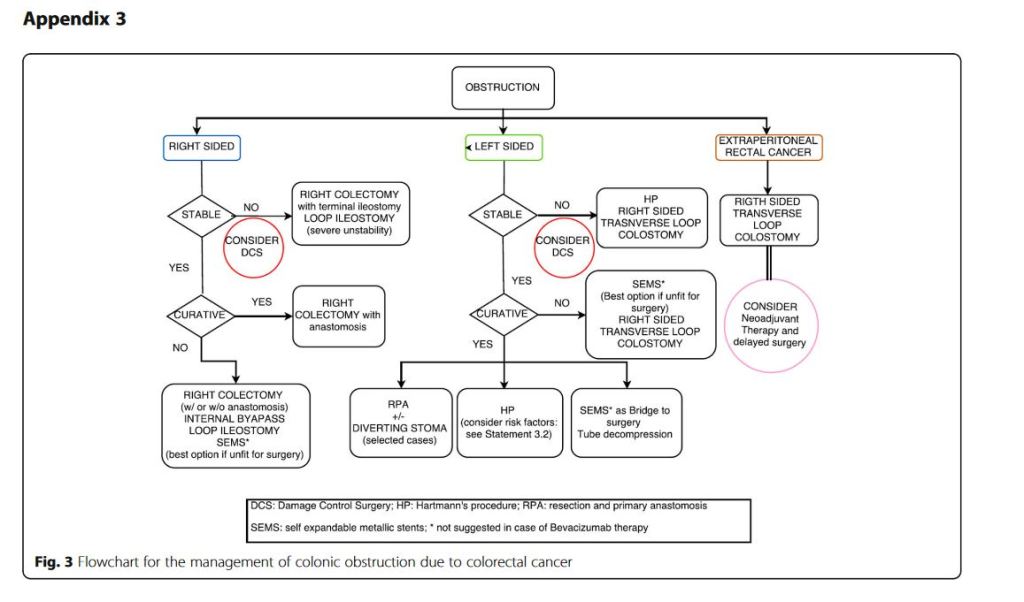
“Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).” “CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann’s procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted. With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.”
“Conclusions: grey areas and opportunities for improvements
We found some limitations within the present guidelines:
– They fail to cover all the possible abdominal scenarios when colon cancer occurs as an emergency: for example, associated resections were not taken into considerations, neither we discussed about therapeutic strategies in case of evidence of peritoneal carcinomatosis. – Despite our attempts to underline suggestions in case of low technical resources, the present guidelines are generally oriented toward hospitals with high level of resources.
On the other side, in our opinion, the current guidelines suggest some stimuli for doctors involved in this field:
– To review the approach to patient suffering from abdominal pain by introducing and promoting the use of bedside abdominal US. – To bear in mind that the emergency surgeon should have a strong oncologic background or that the specialised colorectal surgeon should have a strong background of surgical pathophysiology, emergency surgery and damage control philosophy. – To promote the use of clinical pathways within singular Hospitals”
Results: A total of 755 (out of 844) surgeries in 715 patients were included. Adhesiolysis was required in 475 (62.9%) of operations. Median adhesiolysis time was 20 minutes (range: 1-177). Fifty patients (10.5%) undergoing adhesiolysis inadvertently incurred bowel defect, compared with 0 (0%) without adhesiolysis (P < 0.001). In univariate and multivariate analyses, adhesiolysis was associated with an increase of sepsis incidence [odds ratio (OR): 5.12; 95% confidence interval (CI): 1.06-24.71], intra-abdominal complications (OR: 3.46; 95% CI: 1.49-8.05) and wound infection (OR: 2.45; 95% CI: 1.01-5.94), longer hospital stay (2.06 ± 1.06 days), and higher hospital costs [$18,579 (15,204-21,954) vs $14,063 (12,471-15,655)]. Mortality after adhesiolysis complicated by a bowel defect was 4 out of 50 (8%), compared with 7 out of 425 (1.6%) after uncomplicated adhesiolysis (OR: 5.19; 95% CI: 1.47-18.41).
“Volvulus of the intestines involves twisting around a fixed point. It may occur anywhere along the gastrointestinal tract where there is a long, mobile intestinal segment with a narrow mesenteric attachment. Volvulus leads to luminal obstruction and can compromise intestinal blood flow. For this reason, it tends to be a surgical emergency which requires prompt attention. Failure to recognize the signs and symptoms of intestinal volvulus may lead to bowel ischemia and perforation.”
Results: A total of 2,587 patients were included (2,013 ER, 345 DS, and 229 SEMS). A trend was observed in reversal of ER (decrease from 86.2% to 69.6%) and SEMS (increase from 1.3% to 7.8%) after 2014, with an ongoing increase in DS (from 5.2% in 2009 to 22.7% in 2016). DS after 2014 was associated with more laparoscopic resections (66.0% vs 35.5%; P<.001) and more 2-stage procedures (41.5% vs 28.6%; P=.01) with fewer permanent stomas (14.7% vs 29.5%; P=.005). Overall, more laparoscopic resections (25.4% vs 13.2%; P<.001) and shorter total hospital stays (14 vs 15 days; P<.001) were observed after 2014. However, similar rates of primary anastomosis (48.7% vs 48.6%; P=.961), 90-day complications (40.4% vs 37.9%; P=.254), and 90-day mortality (6.5% vs 7.0%; P=.635) were observed.
CONCLUSIONS: Guideline revision resulted in a notable change from ER to BTS for LSOCC. This was accompanied by an increased rate of laparoscopic resections, more 2-stage procedures with a decreased permanent stoma rate in patients receiving DS as BTS, and a shorter total hospital stay. However, overall 90-day complication and mortality rates remained relatively high.