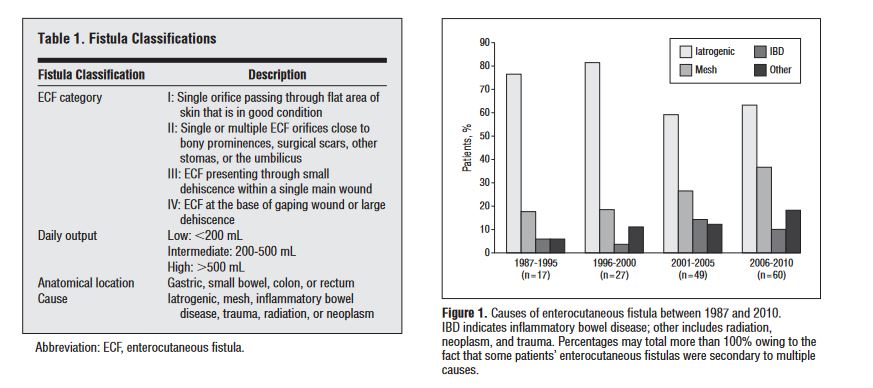
“Enterocutaneous Fistula (ECF) is defined as an abnormal connection between the gastrointestinal tract and the skin, and it requires labor-intensive medical management and surgical expertise. Complex wound management, severe malnutrition, frequent infectious complications, chronic pain, and depression require significant investment of health care resources and make the short-term and long-term care of these patients difficult.”
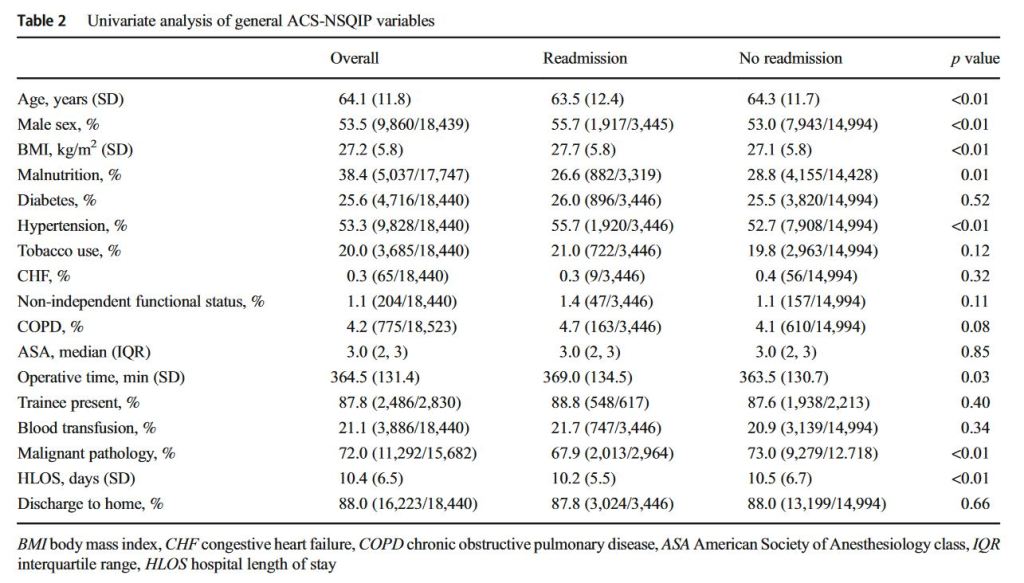
“Readmissions are a common complication after pancreaticoduodenectomy and are increasingly being used as a performance metric affecting quality assessment, public reporting, and reimbursement. This study aims to identify general and pancreatectomy-specific factors contributing to 30-day readmission after pancreaticoduodenectomy, and determine the additive value of incorporating pancreatectomy-specific factors into a large national dataset.” “Large registry analyses of pancreatectomy outcomes are markedly improved by the incorporation of granular procedure-specific data. These data emphasize the need for prevention and careful management of perioperative infectious complications, fluid management, thromboprophylaxis, and pancreatic fistulae.”
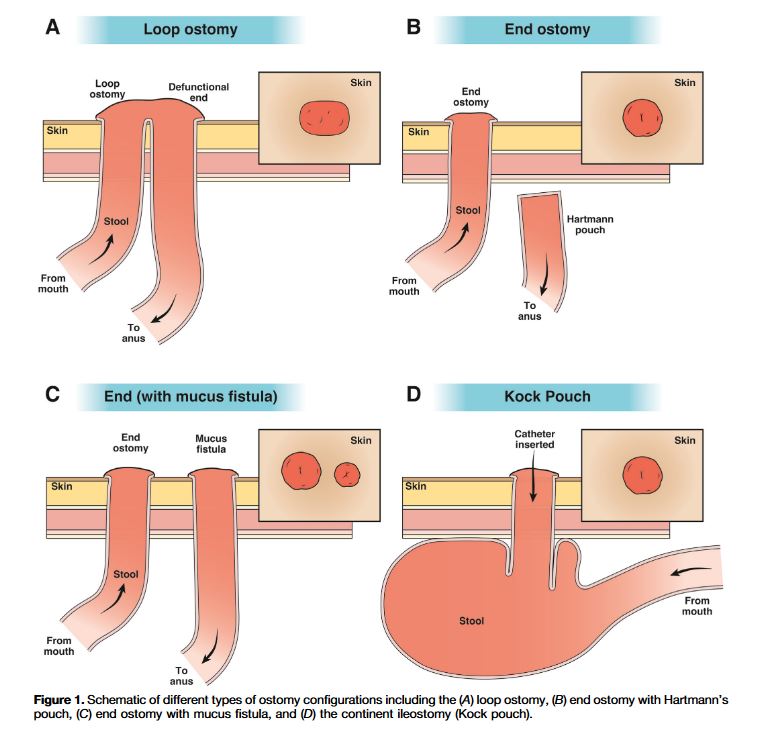
“Enteral ostomies are common in the management of patients with gastrointestinal conditions, including colorectal cancer (CRC), inflammatory bowel disease (IBD), diverticular disease, intestinal trauma, and intestinal perforation. An estimated 750,000 Americans live with an ostomy and 130,000 new ostomy surgeries occur in the United States annually. People with ostomies often face postsurgical complications and challenges to daily self-care. Studies have suggested that adequate stomal care improves clinical outcomes and reduces hospitalizations. However, little guidance exists to support clinicians in managing patients with an ostomy beyond the immediate perioperative period.”
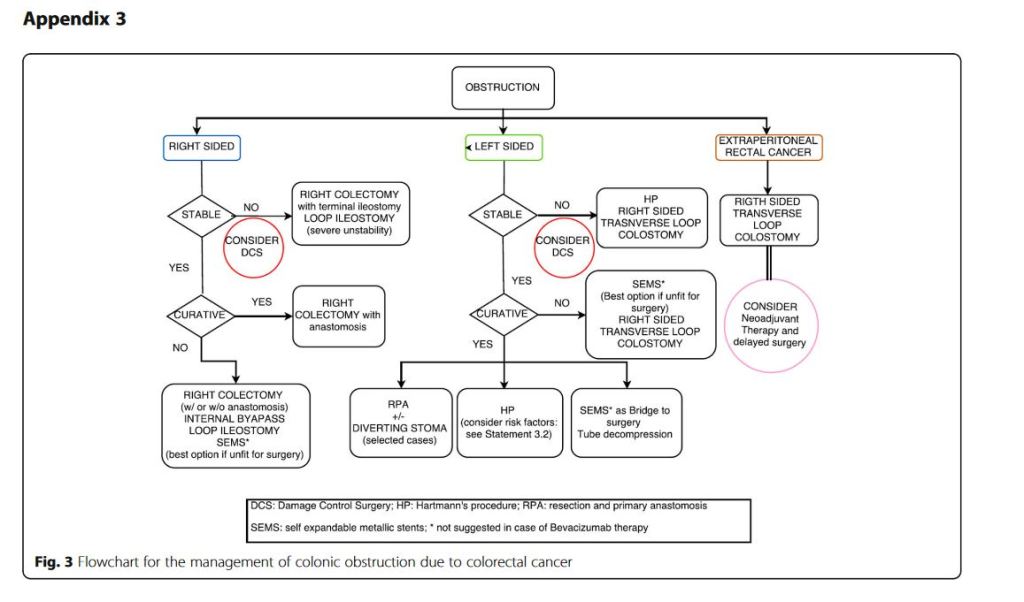
“Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).” “CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann’s procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted. With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.”
“Conclusions: grey areas and opportunities for improvements
We found some limitations within the present guidelines:
– They fail to cover all the possible abdominal scenarios when colon cancer occurs as an emergency: for example, associated resections were not taken into considerations, neither we discussed about therapeutic strategies in case of evidence of peritoneal carcinomatosis. – Despite our attempts to underline suggestions in case of low technical resources, the present guidelines are generally oriented toward hospitals with high level of resources.
On the other side, in our opinion, the current guidelines suggest some stimuli for doctors involved in this field:
– To review the approach to patient suffering from abdominal pain by introducing and promoting the use of bedside abdominal US. – To bear in mind that the emergency surgeon should have a strong oncologic background or that the specialised colorectal surgeon should have a strong background of surgical pathophysiology, emergency surgery and damage control philosophy. – To promote the use of clinical pathways within singular Hospitals”
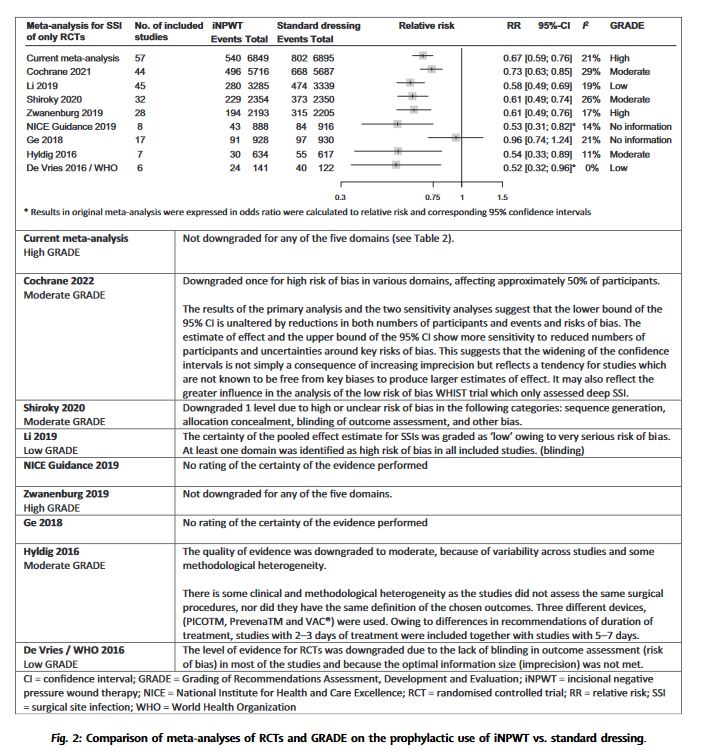
“The evidence on prophylactic use of negative pressure wound therapy on primary closed incisional wounds (iNPWT) for the prevention of surgical site infections (SSI) is confusing and ambiguous. Implementation in daily practice is impaired by inconsistent recommendations in current international guidelines and published meta-analyses. More recently, multiple new randomised controlled trials (RCTs) have been published. This study aimed to provide an overview of all meta-analyses and their characteristics; to conduct a new and up-to-date systematic review and meta-analysis and Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment; and to explore the additive value of new RCTs with a trial sequential analysis (TSA).”
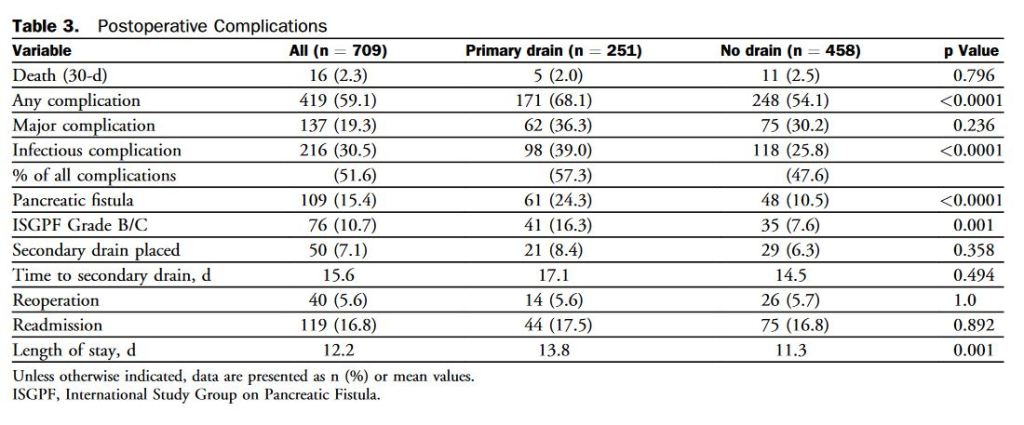
“Postoperative pancreatic fistula (POPF) is a potentially devastating complication after pancreatic resection, seen in 5% to 30% of patients. Depending on severity, POPF may be associated with infectious complications, reoperation, increased length of hospital stay, readmission, and even death. Historically, surgeons placed drains routinely for many abdominal procedures to control potential leaks from various anastomoses. However, this practice has been abandoned by many surgeons over the last 2 decades because no benefit to routine abdominal drainage has been observed from several randomized controlled trials for resections of the colon and rectum, gallbladder, and liver.”
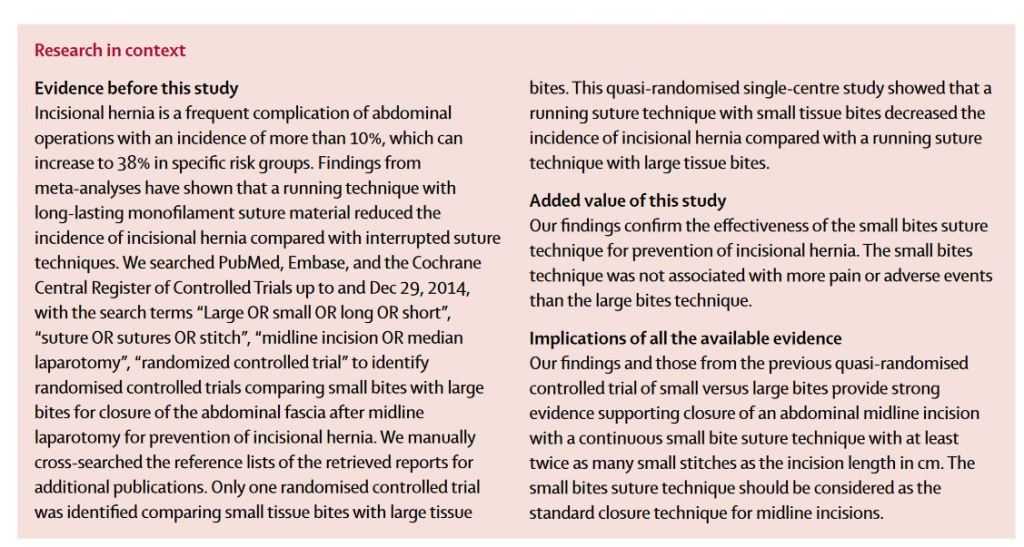
“Incisional hernia is a frequent complication of abdominal operations with an incidence of 10–23%, which can increase to 38% in specific risk groups. In the USA 4 million to 5 million laparotomies are done annually, suggesting that at least 400 000–500 000 incisional hernias can be expected to occur every year. Incisional hernia is associated with pain and discomfort, resulting in a decreased quality of life. Moreover, incarceration and strangulation of abdominal contents can take place, for which emergency surgery is indicated, with associated morbidity and mortality. About 348 000 operations for incisional hernia are done every year in the USA with US$3·2 billion in annual associated costs. Prevention of incisional hernia is therefore of paramount importance.”