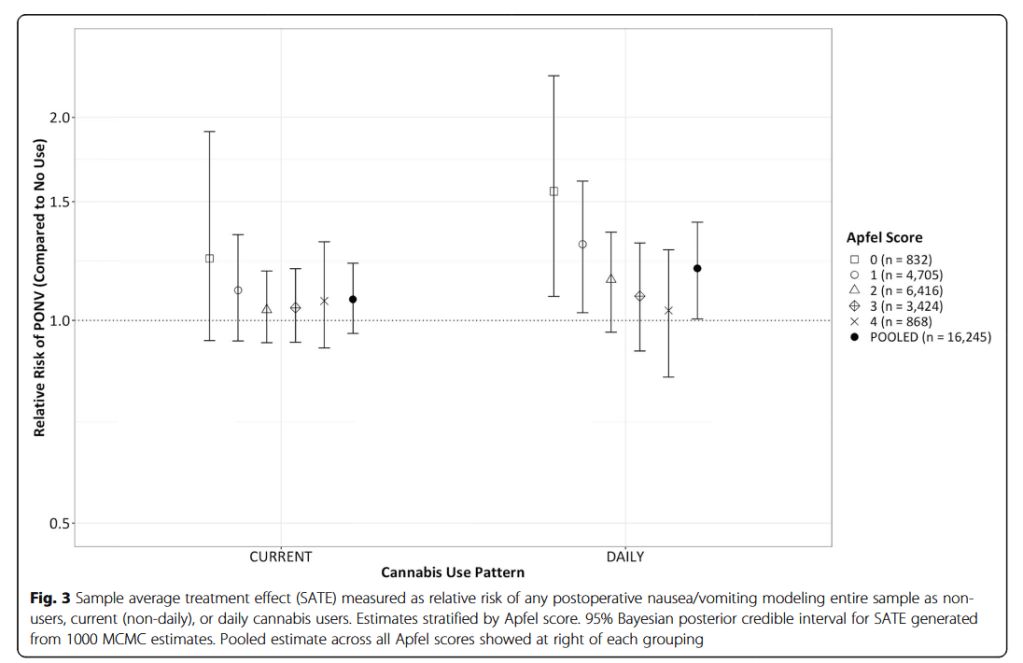
“As cannabinoid compounds have been shown to be effective treatments for chemotherapy induced nausea and vomiting (CINV), it seems reasonable to conjecture that cannabis use could exert a prophylactic or therapeutic effect for patients at risk for or suffering from postoperative nausea and vomiting (PONV). While several studies have examined the role of therapeutically administered cannabinoids in the prevention and treatment of PONV, almost nothing is known about the impact of chronic use of cannabis on the risk for developing PONV. The present investigation examines whether an association exists between patient-described use and/or frequency of cannabis and the occurrence of PONV following general anesthesia.”