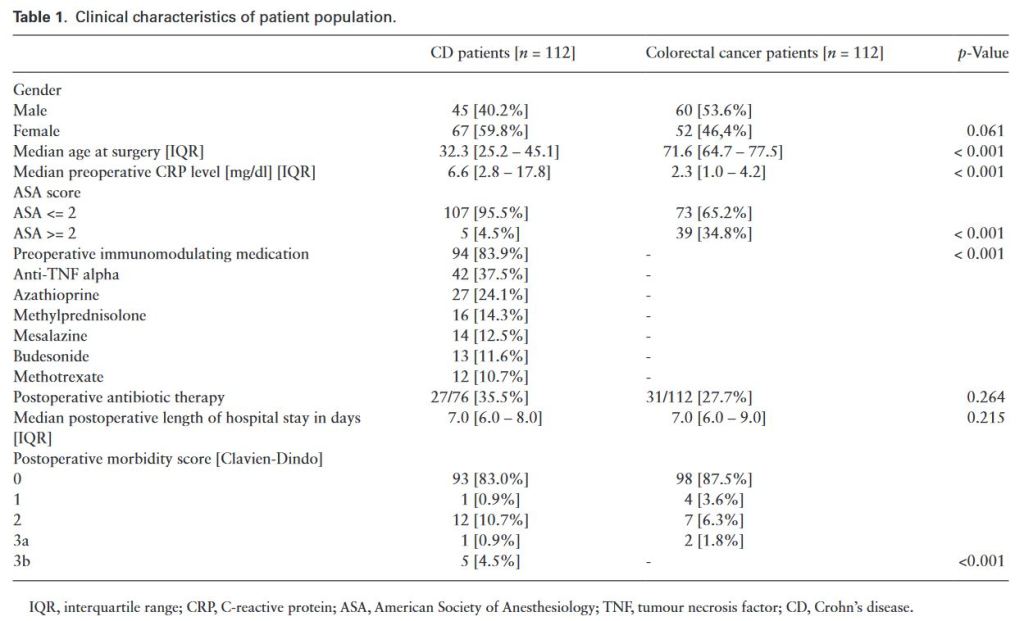
“Crohn’s Disease is an inflammatory bowel disease with a multifactorial pathophysiology. Genetic, immune, gut microbiota, and other environmental factors play a role in the occurrence and maintenance of bowel inflammation. Unfortunately, despite the development of new drugs, about half of all CD patients will need surgery during their disease course.”
“The incidence of biliary injury after laparoscopic cholecystectomy (LC) has shown a declining trend though it may still be twice that as with open cholecystectomy. Major biliary or vasculobiliary injury is associated with significant morbidity. As prevention is the best strategy, the concept of a culture of safe cholecystectomy has been recently introduced to educate surgeons and apprise them of basic tenets of safe performance of LC. Various aspects of safe cholecystectomy include: (1) thorough knowledge of relevant anatomy, various anatomical landmarks, and anatomical variations (2) an understanding of the mechanisms involved in biliary/vascular injury, the most important being the misidentification injury (3) identification of various preoperative and intraoperative predictors of difficult cholecystectomy (4) proper gallbladder retraction (5) safe use of various energy devices (6) understanding the critical view of safety, including its doublet view and documentation (7) awareness of various error traps (e.g., fundus first technique) (8) use of various bailout strategies (e.g., subtotal cholecystectomy) in difficult gallbladder cases (9) use of intraoperative imaging techniques (e.g., intraoperative cholangiogram) to ascertain correct anatomy (10) understanding the concept of time-out.”
“Bile duct injury (BDI) is a dangerous complication of cholecystectomy, with significant postoperative sequelae for the patient in terms of morbidity, mortality, and long-term quality of life. BDIs have an estimated incidence of 0.4–1.5%, but considering the number of cholecystectomies performed worldwide, mostly by laparoscopy, surgeons must be prepared to manage this surgical challenge. Most BDIs are recognized either during the procedure or in the immediate postoperative period. However, some BDIs may be discovered later during the postoperative period, and this may translate to delayed or inappropriate treatments. Providing a specific diagnosis and a precise description of the BDI will expedite the decision-making process and increase the chance of treatment success.”
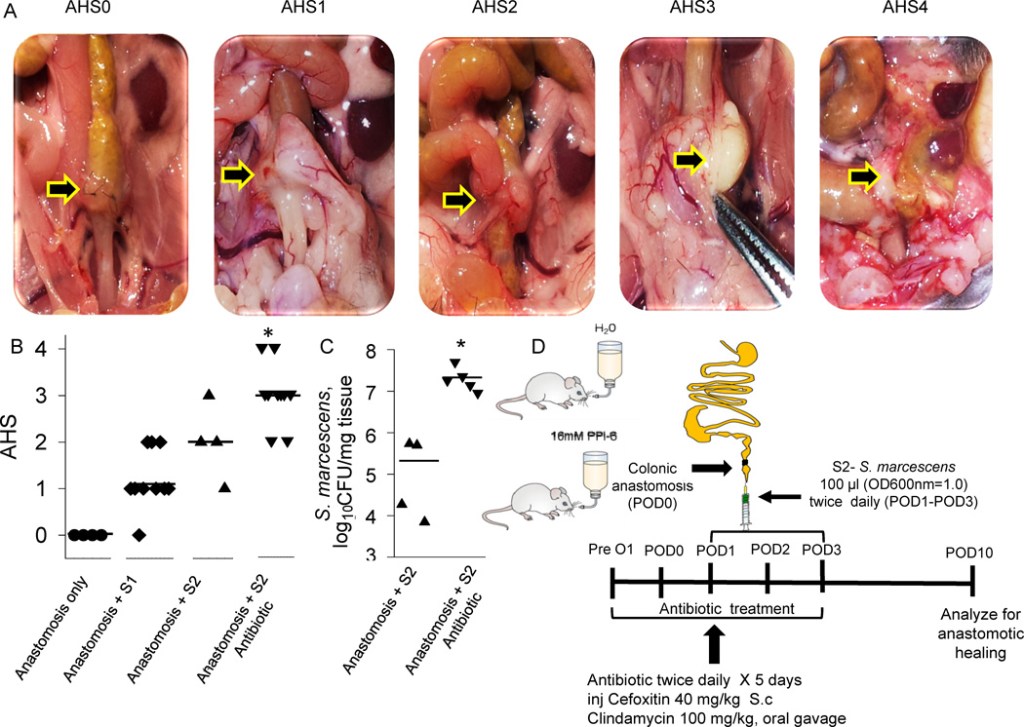
“Despite decades of descriptive research, the etiology and pathogenesis of AL remains unknown. Although there is compelling evidence that microbes are the primary drivers of the pathogenesis of anastomotic leak, few efforts have been aimed at understanding and controlling the microbes that may complicated anastomotic healing.”
“A microbial cause for anastomotic leak was first proposed over 60 years ago and has been confirmed in multiple studies. The main clinical evidence for a microbial cause of anastomotic leak is indirect and is based on clinical trials in which the use of oral non-absorbable antibiotics significantly reduce the incidence of anastomotic leak”
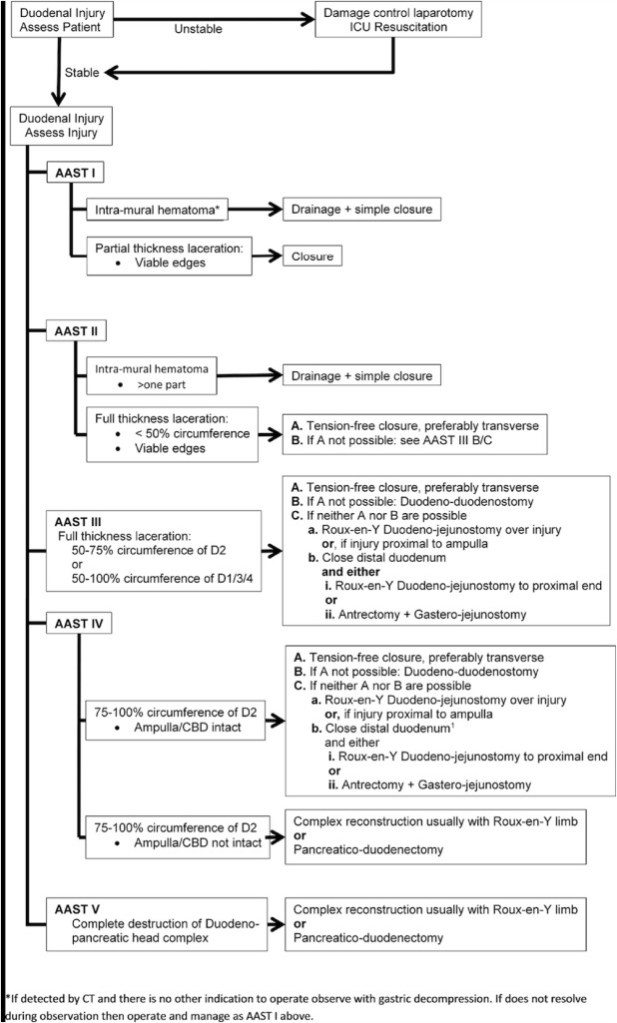
“Duodenal trauma is a rare occurrence existing in 1–4.7% of all abdominal trauma. Its posterior and partially retroperitoneal location shields it from most traumatic mechanisms. Colloquially referred to as the ‘surgical soul’, its proximity to complex regional anatomy makes duodenal trauma particularly at risk for biliary, pancreatic and major vascular injury with 68–86.5% of patients sustaining an associated injury.”
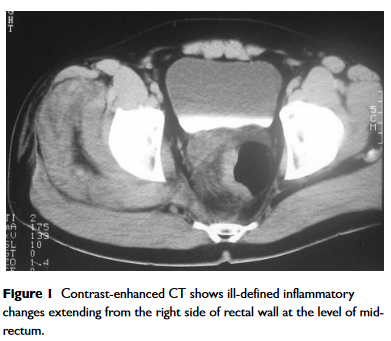
“Perirectal sepsis is a potentially severe complication which may follow minor anorectal intervention and be slow to be diagnosed and treated. Awareness of the possible diagnosis, urgent investigation with cross-sectional imaging and immediate treatment with broad-spectrum antibiotics is vital. However, radical surgical intervention may be necessary.”
Methods: Review of patients from 2002 to 2013 who underwent flexible endoscopy within 6 weeks of creation of gastrointestinal anastomosis. Exclusion criteria included intraoperative endoscopy, anastomotic perforation prior to endoscopy, and endoscopy remote from the anastomotic site. Data are presented as median (interquartile range; IQR) or percentages as appropriate.