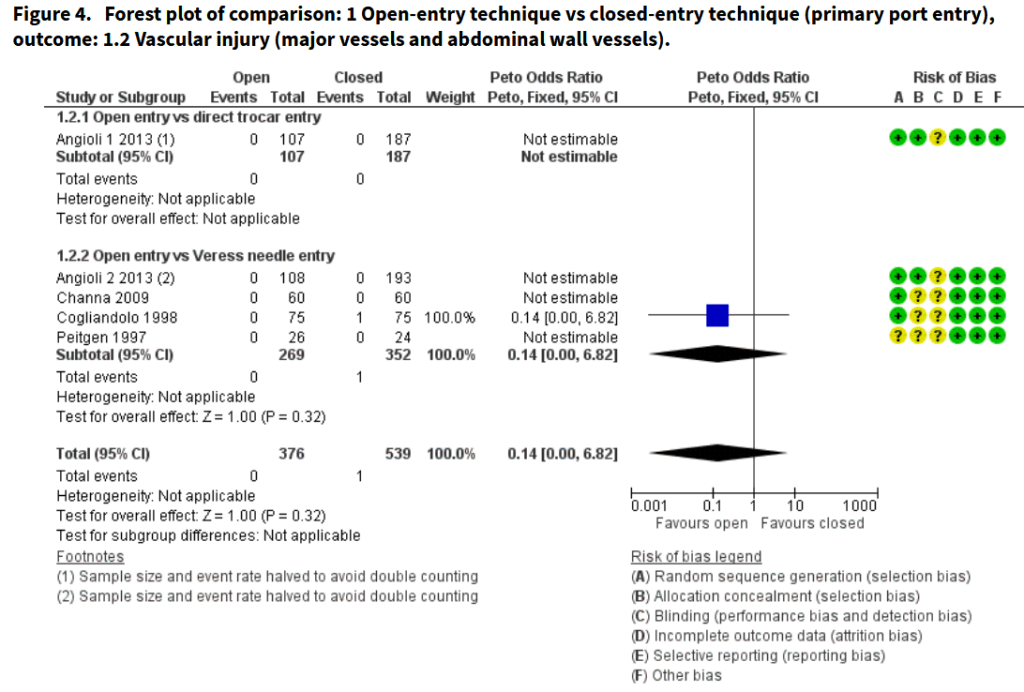
“Laparoscopy is a surgical procedure commonly used in gynaecology whereby a laparoscope is used to gain intra-abdominal access via less extensive incisions. Evidence suggests that laparoscopy provides significant benefits compared to laparotomy in terms of surgical outcomes for patients and costs for healthcare providers. Unlike in conventional open surgery, the surgeon is usually unable to visualise the initial entry into the peritoneal cavity. Most laparoscopic complications occur during the initial entry. These may happen
at several stages including Veress needle insertion, creation of a pneumoperitoneum, and primary trocar insertion. Opinion is divided as to the safest entry technique, and clinical practice is varied. Although gynaecologists commonly use a closed method of entry, other surgical specialties routinely use open methods of entry.”