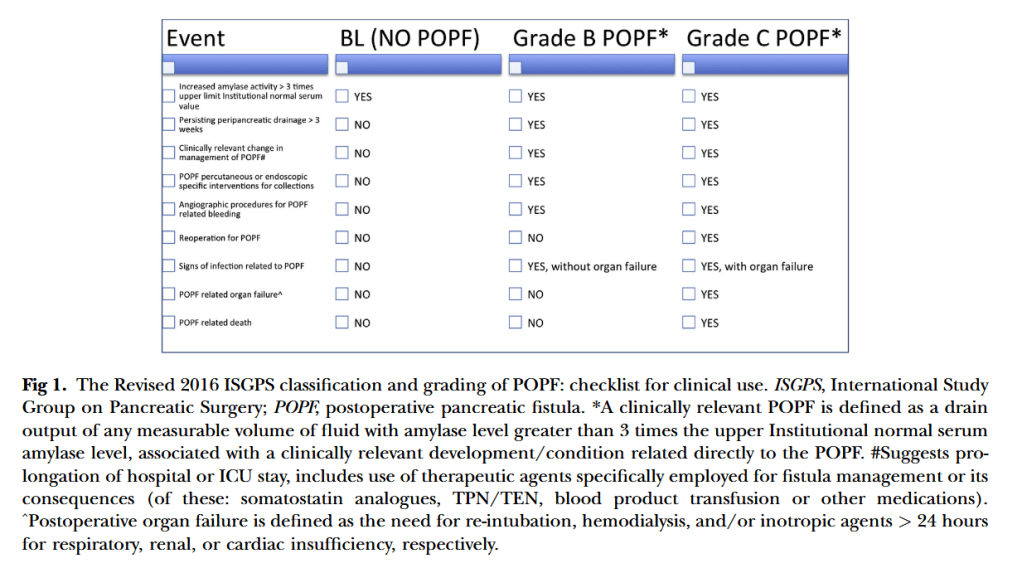
“Based on the literature since 2005 investigating the validity and clinical use of the original
International Study Group of Pancreatic Fistula classification, a clinically relevant postoperative pancreatic fistula is now redefined as a drain output of any measurable volume of fluid with an amylase level >3 times the upper limit of institutional normal serum amylase activity, associated with a clinically relevant development/condition related directly to the postoperative pancreatic fistula. Consequently, the former “grade A postoperative pancreatic fistula” is now redefined and called a “biochemical leak,” because it has no clinical importance and is no longer referred to a true pancreatic fistula. Postoperative pancreatic fistula grades B and C are confirmed but defined more strictly. In particular, grade B requires a change in the postoperative management; drains are either left in place >3 weeks or repositioned through endoscopic or percutaneous procedures. Grade C postoperative pancreatic fistula refers to those postoperative pancreatic fistula that require eoperation or lead to single or multiple organ failure and/or mortality attributable to the pancreatic fistula.”