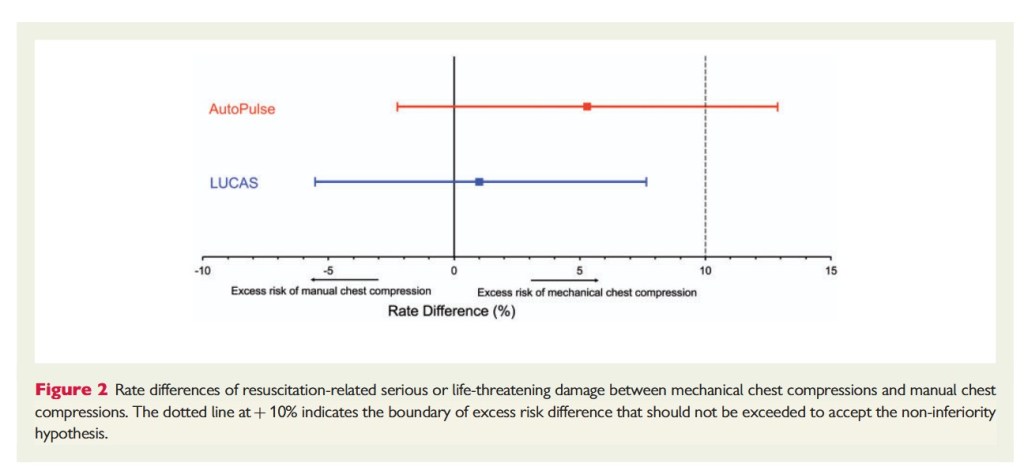
“Mechanical chest compression devices are designed to perform chest compressions at specified rate and depth and therefore were expected to improve outcome. There are at
present two widely used and Food and Drug Administration-approved devices: the AutoPulse, a load-distributed band device that rhythmically compresses and restricts the chest wall and the LUCAS, a piston device with a cup that is placed in the centre of the chest and pushes the sternum down over a distance of 5.2 cm and pulls back to the neutral position. Significant improvement of aortic blood pressure and coronary perfusion pressure is documented in humans from the AutoPulse compared with manual chest compressions. Chest compression with LUCAS resulted in significantly higher end-tidal carbon dioxide in humans compared with manual chest compressions. For several years, only one randomized clinical trial with the AutoPulse was available (ASPIRE), which was terminated after interim analysis because of a trend to reduced survival to discharge compared with manual control CPR. None of the more recent randomized clinical trials demonstrated survival benefit of AutoPulse or LUCAS over manual controls. Anecdotal and possibly biased observations in our hospital and a published letter suggested increased
damage caused by mechanical chest compression devices.”