“Hemorrhoids are vascular structures that arise from a channel of arteriovenous connective tissues and drain into the superior and inferior hemorrhoidal veins. Although hemorrhoids are categorized as external or internal based on their relationship with the dentate line, they communicate with one another and often coexist. Symptoms related to hemorrhoids are very common in the Western hemisphere and other industrialized societies. Although published estimates of prevalence vary, hemorrhoidal disease represents one of the most common medical and surgical disease processes encountered in the United States, resulting in more than 2.2 million outpatient evaluations per year. Many diverse symptoms may be, correctly or incorrectly, attributed to hemorrhoids by both patients and referring physicians. As a result, it is important to identify symptomatic hemorrhoids as the underlying source of the anorectal report and to have a clear understanding of the evaluation and management of this disease process. These guidelines address diagnostic and therapeutic modalities in the management of hemorrhoidal disease.”
“A surgical site infection (SSI) is defined as an infection of the incision (superficial SSI), the tissue below the incision (deep SSI), or within the abdominal cavity (organ space SSI). SSI accounts for more than 20% of all health care-associated infections and is the most common infection after surgery, affecting an estimated 300,000 patients annually. Compared with other surgical subspecialties, patients undergoing colorectal surgery are at the highest risk for developing an SSI with an estimated incidence of 5% to 30%. Patients undergoing emergency colorectal surgery with colon perforation have an SSI incidence as high as 80%.”
TABLE 2.
Summary and strength of GRADE recommendations for preventing SSIs
Summary
Recommendation strength
GRADE quality of evidence
1
Implementing an SSI bundle for patients undergoing colorectal surgery can decrease the incidence of SSI
Strong
Moderate
2
Oral antibiotics in combination with mechanical bowel preparation have been shown to decrease the incidence of SSI after elective colorectal resection
Strong
Moderate
3
In circumstances where a mechanical bowel preparation is contraindicated or otherwise omitted, preoperative oral antibiotic preparation alone can reduce the incidence of SSI
Conditional
Moderate
4
Showering with chlorhexidine before colorectal surgery does not significantly impact SSI rates
Strong
Moderate
5
Smoking cessation before surgery may be recommended to reduce the risk of SSI
Conditional
Moderate
6
On the day of colorectal surgery, patients should have their hair removed from the surgical site using a clipper or not removed at all. Shaving with a razor before surgery is discouraged
Strong
Moderate
7
Patients undergoing colorectal resection should have parenteral antibiotics administered within 60 min of incision. Dosing and redosing should be based on the pharmacokinetic profile of the antibiotic
Strong
Low
8
Patients who report a penicillin allergy may be evaluated for having true hypersensitivity and high-risk reactions to penicillin. Delabeling a penicillin-allergic patient can facilitate the appropriate use of a preoperative prophylactic beta-lactam antibiotic and improve outcomes
Conditional
Low
9
For most clean and clean-contaminated cases, prophylactic parenteral antibiotics should be limited to the initial 24 h postoperatively
Strong
Moderate
10
Cleansing the surgical site with chlorhexidine–alcohol-based preparation is typically recommended for patients undergoing colorectal surgery
Strong
Moderate
11
Hyperglycemia on the day of surgery and in the immediate postoperative period may increase the risk of SSI after elective colorectal resection
Conditional
Moderate
12
Maintaining intraoperative normothermia may decrease the incidence of SSI in patients undergoing colorectal surgery
Conditional
Low
13
High-fractionated oxygen is not routinely recommended to prevent SSI
Conditional
Moderate
14
Wound protectors can decrease the incidence of SSI after colorectal surgery
Strong
High
15
Minimally invasive colorectal surgery can decrease the incidence of SSI compared to open surgery
Strong
High
16
Topical antimicrobial agents applied to the surgical incision are not recommended
Strong
Low
17
NPWT for primarily closed incisions may decrease the incidence of SSI
Conditional
Moderate
18
Advanced silver or antimicrobial dressings are not routinely recommended for clean or clean-contaminated wounds after colorectal surgery
Conditional
Moderate
GRADE = Grading of Recommendations, Assessments, Development, and Evaluation; NPWT = Negative pressure wound therapy; SSI = surgical site infection.
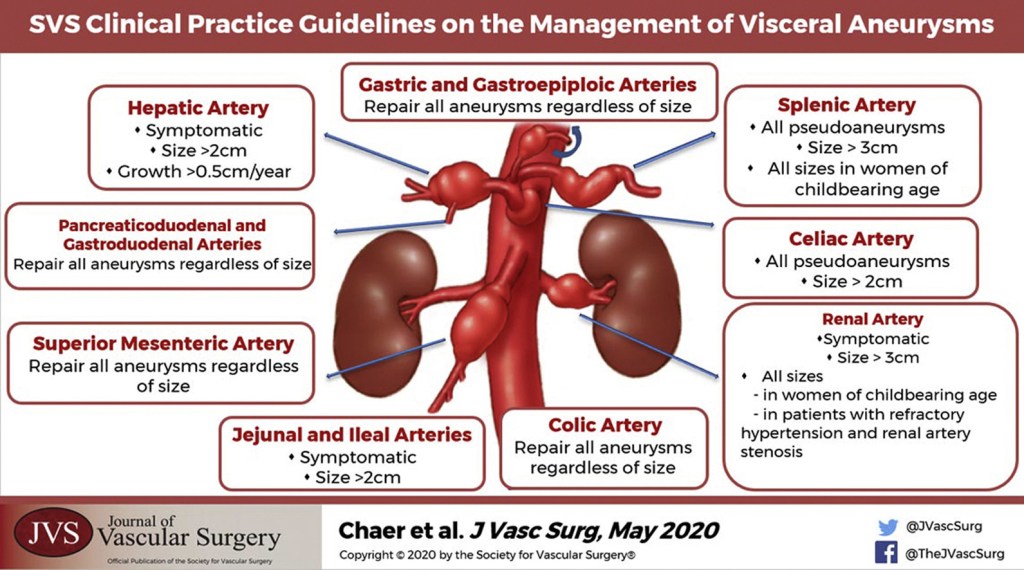
“Although not directed by randomized prospective trials, general principles of management of visceral artery aneurysms do exist. Because of their potential for rupture, most visceral artery pseudoaneurysms, mycotic aneurysms, and many larger true aneurysms warrant intervention. Treatment can generally be accomplished by either open surgical or endovascular approaches. The treatment goal is to prevent aneurysm expansion and potential rupture by exclusion from the arterial circulation while maintaining necessary distal or collateral bed perfusion. Depending on the location of the aneurysm, this can be accomplished in a variety of ways. In areas of the visceral circulation with an abundance of collateral flow, for example, in the splenic artery, proximal and distal ligation of the aneurysm segment is a viable surgical option. This can also be accomplished with endovascular isolation of the aneurysmal segment, either by placement of a stent graft or by coil embolization of the proximal and distal arterial segment. The preferred treatment of an individual patient and aneurysm must be carefully based on the particular anatomy and any associated clinical conditions as well as the underlying condition of the patient. The purpose of these guidelines is to inform the diagnosis, treatment options, screening, and follow-up of visceral aneurysms based on the available published literature and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach”
“Popliteal artery aneurysms (PAAs) are the most common peripheral arterial aneurysms, defined as aneurysms outside the aortoiliac system or the brain, accounting for 70% of all peripheral arterial aneurysms. They are more common in men (95%) and tend to occur in the sixth and seventh decades of life. Few modern studies have been performed on the natural history of PAAs, and many of these were retrospective reviews of surgical patients. As such, the timing and details of PAA management remain nuanced.”
“These guidelines focus on PAA screening, indications for intervention, choice of repair strategy, management of asymptomatic and symptomatic PAAs (including those presenting with acute limb ischemia), and follow-up of both untreated and treated PAAs. They offer long-awaited evidence-based recommendations for physicians taking care of these patients.”