A multivariate analysis showed the following adverse risk factors for AL: age > 65 years, hemoglobin < 8.0 g/dL and malnourishment. A multivariable model for AL showed a strong optimism-adjusted discrimination (concordance index, 0.675).


A multivariate analysis showed the following adverse risk factors for AL: age > 65 years, hemoglobin < 8.0 g/dL and malnourishment. A multivariable model for AL showed a strong optimism-adjusted discrimination (concordance index, 0.675).
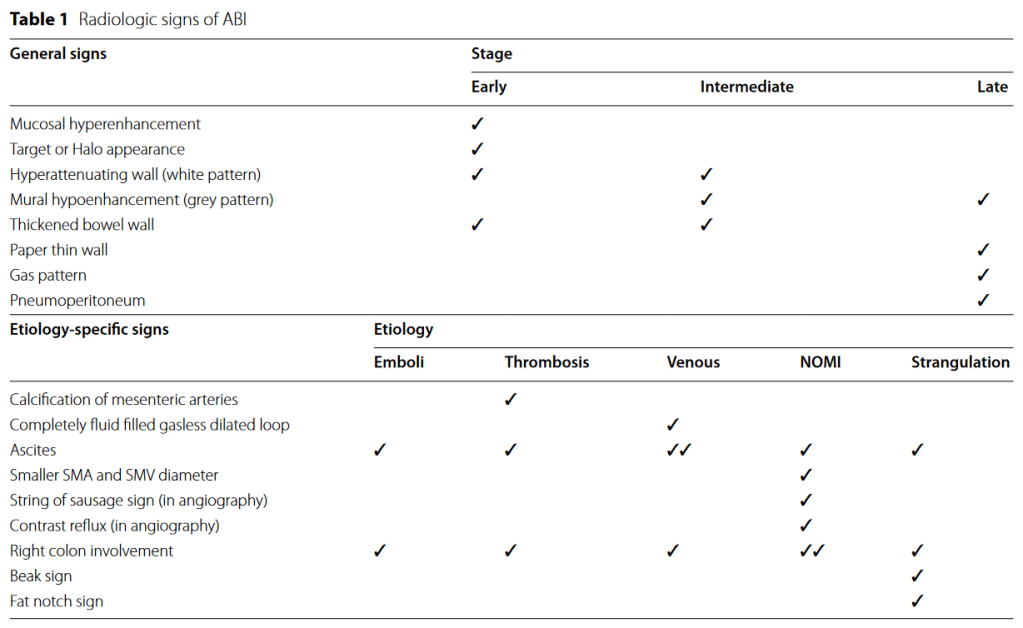
“Acute bowel ischemia (ABI) can be life threatening with high mortality rate. The radiologist plays a central role in the initial diagnosis and preventing progression to irreversible intestinal ischemic injury or bowel necrosis. The most single imaging findings described in the literature are either non-specific or only present in the late stages of ABI, urging the use of a constellation of features to reach a more confident diagnosis”
Mirrielees JA, et al. Pancreatic Fistula and Delayed Gastric Emptying Are the Highest-Impact Complications After Whipple. J Surg Res. 2020 Jun;250:80-87.
Full-text for Emory users.
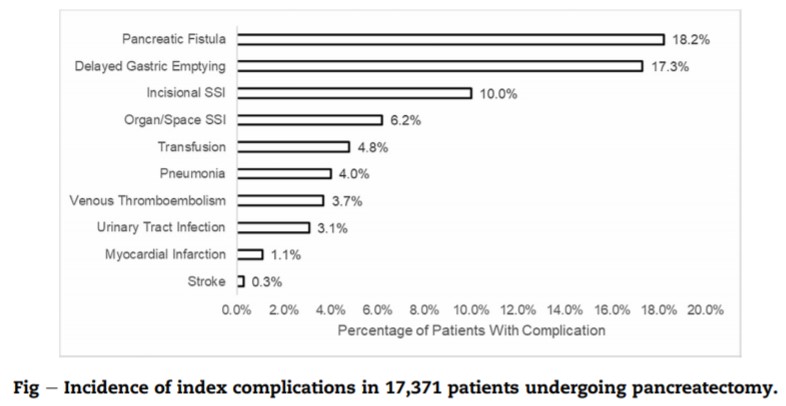
Results: About 10,922 patients undergoing pancreaticoduodenectomy were included for analysis. The most common postoperative complications were DGE (17.3%), POPF (10.1%), incisional SSI (10.0%), and organ/space SSI (6.2%). POPF and DGE were the only complications that demonstrated sizable effects for all clinical and resource utilization outcomes studied. Other complications had sizable effects for only a few of the outcomes or had small effects for all the outcomes.
Continue readingDumon K, Dempsey DT. (2019). Postgastrectomy Syndromes. Shackelford’s Surgery of the Alimentary Tract, 8th ed.: 719-734.
“Hypergastrinemia after distal gastrectomy can be caused by gastrinoma or retained antrum. In the latter there is residual antral tissue left in continuity with the duodenal stump after gastric resection with Billroth II anastomosis. The G cells in this retained antral tissue are not exposed to luminal acid, resulting in continuous secretion of gastrin and intense stimulation of acid production by parietal cells in the proximal gastric remnant. The exposure of the unbuffered jejunum to this high acid level at the Billroth II GJ results in marginal ulcer (see Fig. 62.12B ).
Continue readingNishizaki D, Ganeko R, Hoshino N, et al. Roux-en-Y versus Billroth-I reconstruction after distal gastrectomy for gastric cancer. Cochrane Database Syst Rev. 2021 Sep 15;9(9): CD012998.
Matsumoto K, Tanaka S, Toyonaga T, et al. Clinical Impact of Different Reconstruction Methods on Remnant Gastric Cancer at the Anastomotic Site after Distal Gastrectomy. Clin Endosc. 2021 Aug 13. Epub ahead of print.
Continue readingHarriman S, Rodych N, Hayes P, Moser MA. The C-reactive protein-to-prealbumin ratio predicts fistula closure. Am J Surg. 2011 Aug;202(2):175-8.
Full-text for Emory users.
Background: The purpose of this study was to evaluate the predictability of fistula closure using the ratio of C-reactive protein to prealbumin (C:P ratio).
Methods: A database of 89 patients with gastrointestinal fistulas (1994-2009) was created based on the records of our Nutrition Support Services Team. All patients had weekly blood work including C-reactive protein level, prealbumin level, and albumin level. Forty-three fistulas were managed without surgery for 6 weeks or more; of these, 29 closed.
Continue readingJolissaint JS, et al. Timing and Outcomes of Abdominal Surgery in Neutropenic Patients. J Gastrointest Surg. 2019 Apr;23(4):643-650.
Full-text for Emory users.
Results: Amongst 237 patients, mortality was 11.8% (28/237) and morbidity 54.5% (130/237). Absolute neutrophil count < 500 cells/μL (50% vs. 20.6%, P < 0.01) and perforated viscus (35.7% vs. 14.8%, P = 0.01) were associated with mortality. Perforated viscus (25.4% vs. 7.5%) was also associated with morbidity. Urgent operations were associated with higher morbidity (63.6% vs 34.7%, P < 0.001) and mortality (16.4% vs 1.4%, P = 0.002) when compared to elective operations. Transfer from an outside hospital (22.3% vs. 11.2%, P = 0.02) and longer median time from admission to operation (2 days (IQR 0-6) vs. 1 day (IQR 0-3), P < 0.01) were associated with morbidity. An ANC threshold of 350 provided the best discrimination for mortality.
Conclusions: Elective surgery in the appropriately chosen neutropenic patient is relatively safe. For patients with obvious surgical pathology, we advocate for earlier operation and a lower threshold for surgical consultation in an effort expedite the diagnosis and necessary treatment.
Continue reading