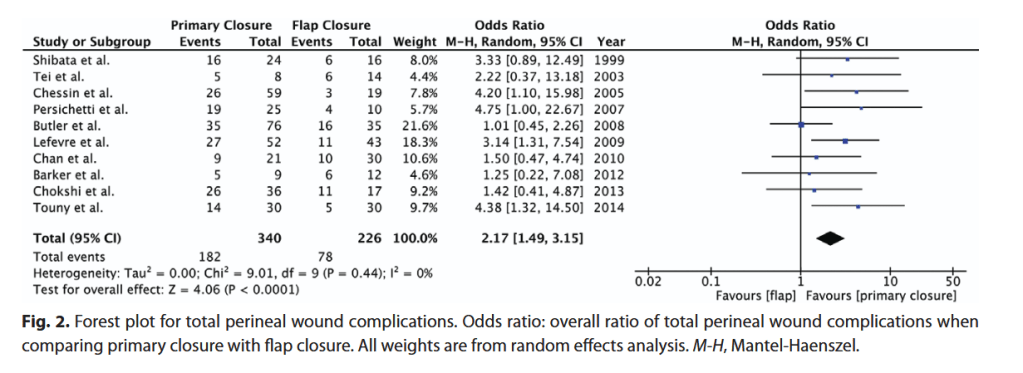
“Abdominoperineal resection and pelvic exenteration for resection of malignancies can lead to large perineal defects with significant surgical-site morbidity. Myocutaneous flaps have been proposed in place of primary closure to improve wound healing. A systematic review was conducted to compare primary closure with myocutaneous flap reconstruction of perineal defects following abdominoperineal resection or pelvic exenteration with regard to surgical-site complications.”
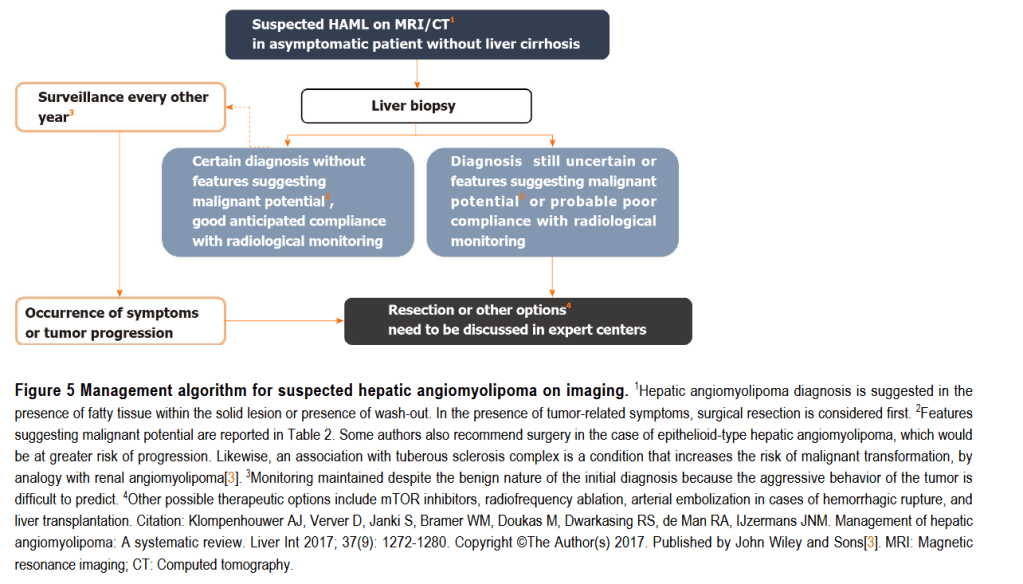
“Angiomyolipoma (AML) is a solid mesenchymal tumor, mainly described in the kidney, and belongs to the group of perivascular epithelioid cell tumors (PEComas). Hepatic localization of AML, described for the first time in 1976, is rare, since only around 600 cases were reported after an exhaustive search of the literature up to the year 2017. Hepatic AML (HAML) poses a veritable diagnostic challenge in radiological terms, especially when fat content is low, because this type of tumor may appear as a hypervascular tumor associated with a washout phase that mimics other, more common hypervascular hepatic tumors, such as hepatocellular carcinoma”
“The reported complication rates after breast cancer surgery are low, with rates ranging from 2% to 50%, and are reportedly more common when performed in conjunction with axillary surgery and immediate breast reconstruction. A breakdown by procedure type has shown morbidity rates between 5% and 50% after mastectomy and from 3% to 35% after lumpectomy with or without reconstruction.”
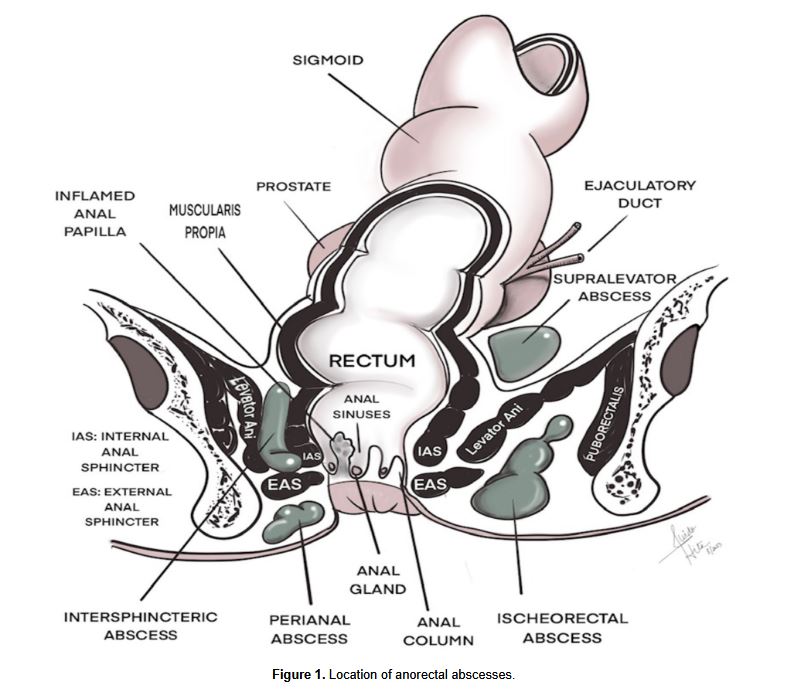
“Anorectal infections in neutropenic leukemia patients are a significant and potentially life-threatening complication. The pathogenesis of this condition is not entirely understood and believed to be multifactorial, including mucosal injury as a result of cytotoxic drugs, profound neutropenia and impaired host defense. Establishing an early diagnosis is key and often made clinically on the basis of signs and symptoms, but also from imaging studies demonstrating perianal inflammation or fluid collection. The management of anorectal infections in neutropenic leukemia patients is not straightforward, as there are no well-conducted studies on this entity.”
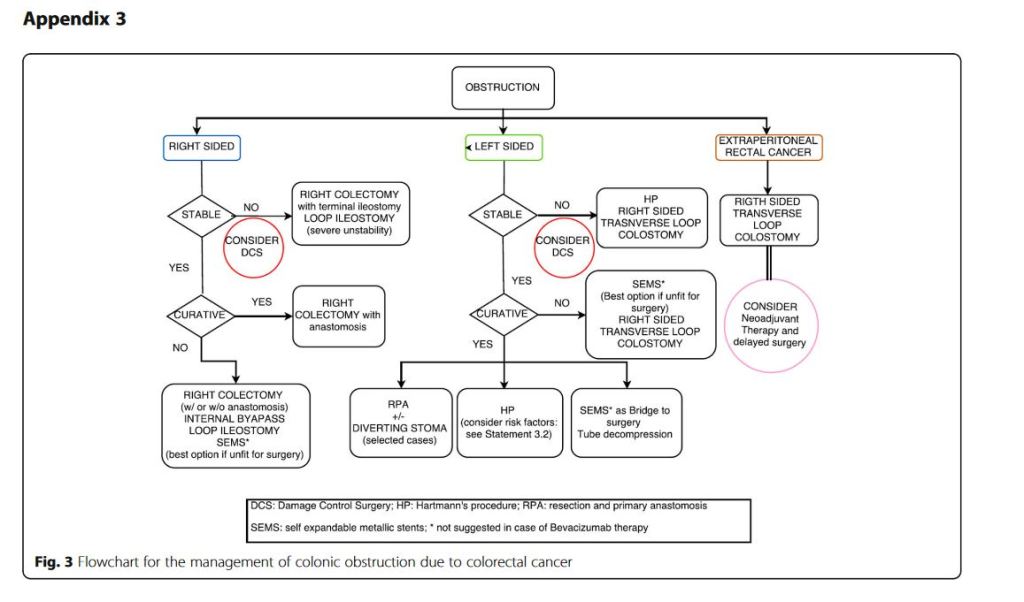
“Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).” “CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann’s procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted. With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.”
“Conclusions: grey areas and opportunities for improvements
We found some limitations within the present guidelines:
– They fail to cover all the possible abdominal scenarios when colon cancer occurs as an emergency: for example, associated resections were not taken into considerations, neither we discussed about therapeutic strategies in case of evidence of peritoneal carcinomatosis. – Despite our attempts to underline suggestions in case of low technical resources, the present guidelines are generally oriented toward hospitals with high level of resources.
On the other side, in our opinion, the current guidelines suggest some stimuli for doctors involved in this field:
– To review the approach to patient suffering from abdominal pain by introducing and promoting the use of bedside abdominal US. – To bear in mind that the emergency surgeon should have a strong oncologic background or that the specialised colorectal surgeon should have a strong background of surgical pathophysiology, emergency surgery and damage control philosophy. – To promote the use of clinical pathways within singular Hospitals”
“Because most patients die from progressive disease in the liver, hepatic arterial infusion pump (HAIP) chemotherapy with floxuridine is an attractive treatment option for unresectable [Intrahepatic cholangiocarcinoma] iCCA. The rationale for HAIP chemotherapy is that iCCA relies mostly on arterial blood supply. Moreover, floxuridine, also known as FUDR, is characterized by its high first-pass effect; approximately 95% is directly metabolized in the liver. Hence, this allows for an up to 400-fold dose increase in subsequent intratumoral exposure compared with systemic treatment, with minimal systemic exposure and side effects”
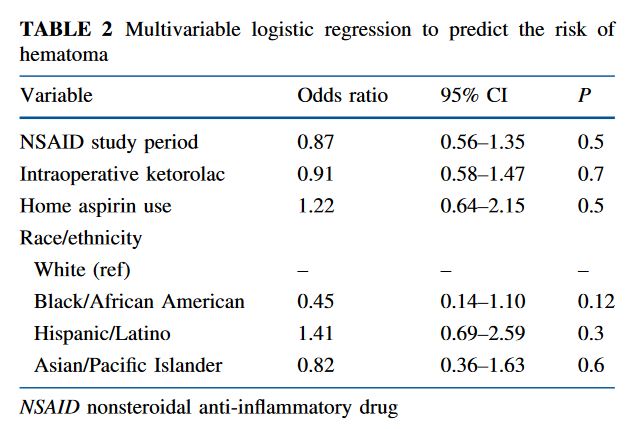
“Among patients undergoing lumpectomy and Sentinel Lymph Node Biopsy with multimodal analgesia, the risk of hematoma in the 30-day postoperative period, including hematoma requiring reoperation and in-office aspiration or drainage, was low overall and not statistically significantly higher despite increased use of intraoperative ketorolac and implementtion of a standard discharge regimen of NSAIDs in lieu of opioids.”