Case Presentation: “A 60-year-old male has been in the post-anesthetic care unit (PACU) for 6 hours with a slowly expanding neck hematoma following an uneventful left carotid endarterectomy under general anesthesia.”
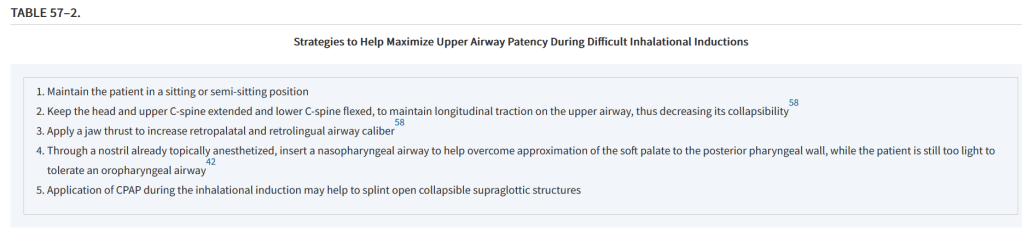

Case Presentation: “A 60-year-old male has been in the post-anesthetic care unit (PACU) for 6 hours with a slowly expanding neck hematoma following an uneventful left carotid endarterectomy under general anesthesia.”
“In endocrine surgery, thyroidectomy is the most frequently performed surgical procedure.
Morbidity related to thyroidectomy is mainly represented by hypoparathyroidism, recurrent laryngeal nerve injury, and cervical haematoma. These complications can occur at a
considerable rate even if thyroid surgery is performed by highly experienced surgeons.
Obtaining accurate haemostasis during thyroidectomy is crucial to prevent the occurrence of postoperative bleeding and, allowing adequate vision of the anatomical structures, is also important to avert the onset of the other complications.”

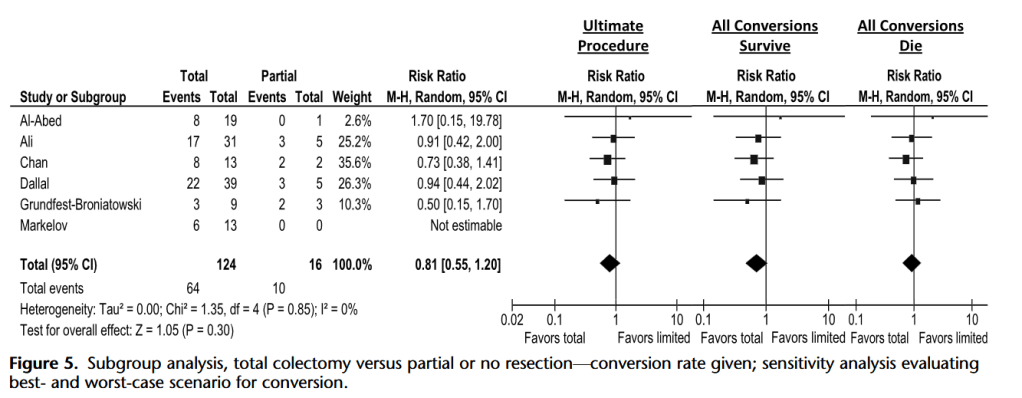
“Findings in the literature suggest that prompt surgical treatment of patients with fulminant Clostridium difficile-associated disease (CDAD) is necessary to ensure patient survival. However, controversy remains regarding the best surgical approach and timing. Recent efforts have been made in the creation of a scoring system to predict deterioration and improve patient care. New surgical approaches such as ileostomy and washout have shown promising results, but more rigorous data and longer follow-up, especially with regard to
disease recurrence after ileostomy reversal, are needed to evaluate the true value of these techniques regarding mortality.”
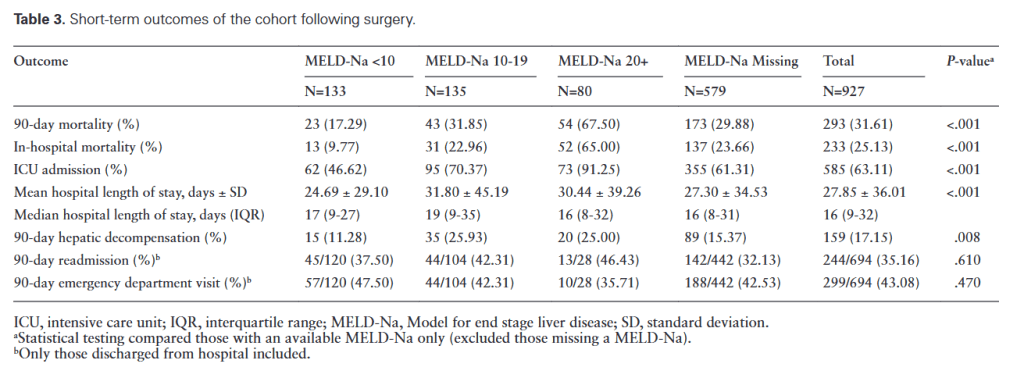
“Individuals with cirrhosis have higher post-operative morbidity and mortality following major abdominal surgery compared to those without cirrhosis. To quantify this added risk, observational studies and prediction models have been described; however, the majority were derived from historic cohorts and may not reflect the changing epidemiology of
liver disease or advances in both the medical management of cirrhosis and perioperative practices in this high-risk group.”
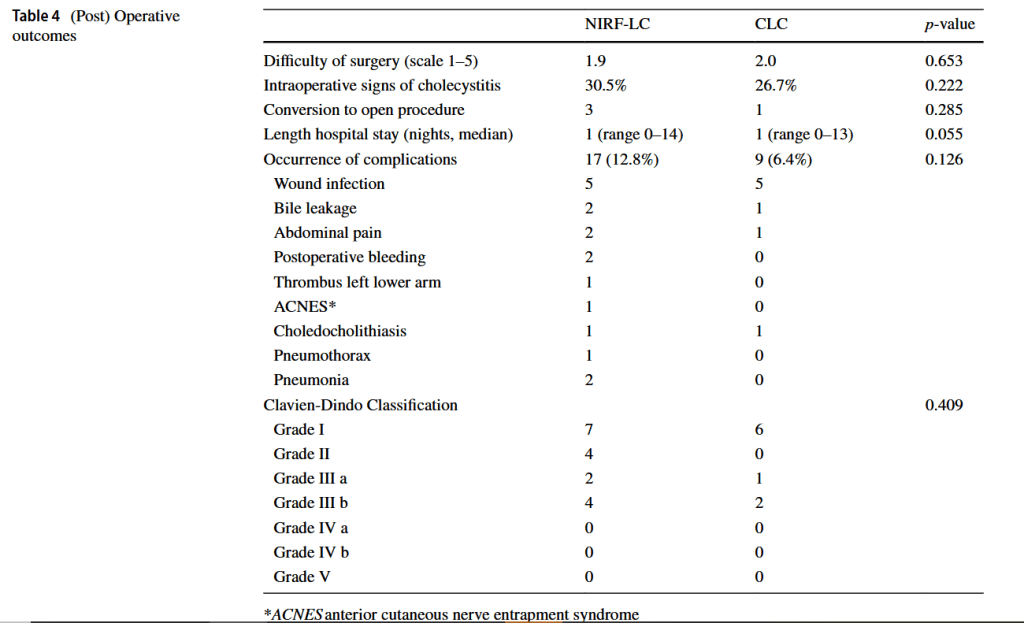
“The most feared complication during laparoscopic cholecystectomy is bile duct injury. Bile duct injury as a result of laparoscopic cholecystectomy is rare with an incidence of 0.3–0.7% but often results in severe morbidity and even mortality, lower quality of life and extra costs.
Misidentification of extra-hepatic bile duct anatomy during laparoscopic cholecystectomy is the main cause of bile duct injury. Examples of such misidentification are mistaking the common bile duct for the cystic duct and aberrant hepatic ducts for the cystic duct or cystic artery. In order to reduce the risk of bile duct injury, techniques to enhance proper identification of the anatomy are needed.”
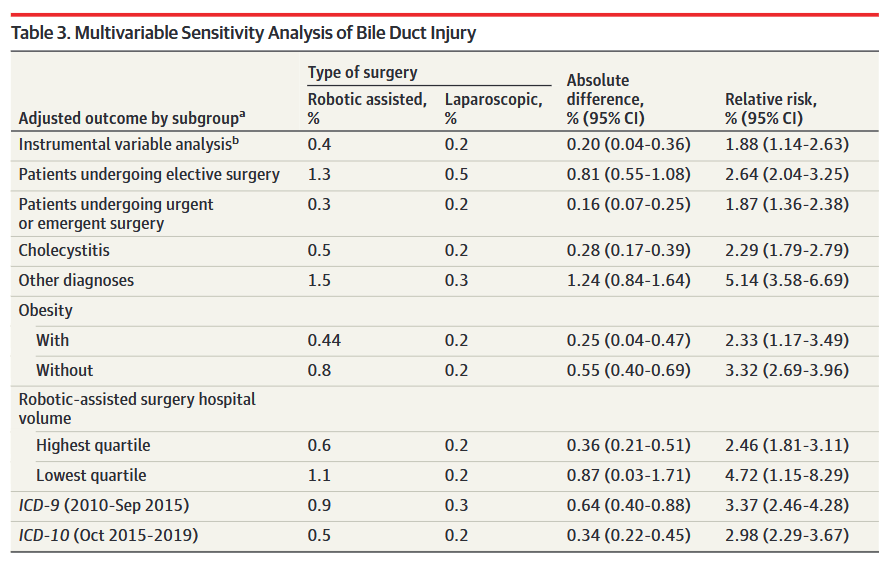
“Whether robotic-assisted cholecystectomy leads to even safer outcomes than minimally invasive laparoscopic cholecystectomy remains unclear. Some contend that robotic-
assisted cholecystectomy may be safer because it offers 3-dimensional visualization, enhanced instrument articulation to allow for more complex maneuvers, novel ways to
visualize biliary anatomy, and potentially increases a surgeon’s ability to perform difficult procedures in a minimally invasive fashion. Studies comparing the safety of these
approaches found equivalency, but are limited to single-center case series inclusive of surgeons with the most robotic-assistance experience. Whether those outcomes reflect
current surgical practice, especially as robotic-assisted cholecystectomy is adopted by a larger and potentially more novice group of surgeons, represents crucial information for
surgeons, referring physicians, and patients.”
“Robotic cholecystectomy was independently associated with a lower risk of serious complications, lower rate conversion to open, and hospitalization ≥24 hours compared with laparoscopic cholecystectomy. These findings suggest that new technologies might enhance the safety of minimally invasive surgery.”
Continue reading