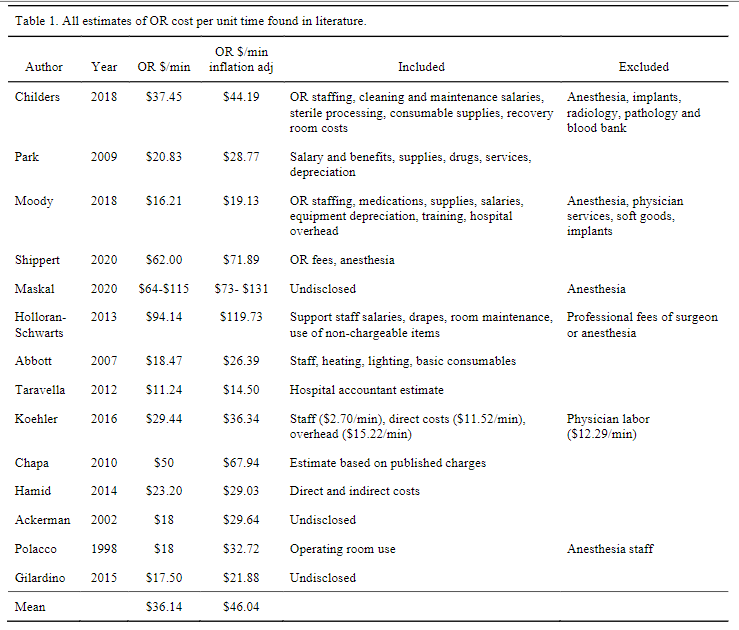
“The cost to run an operating room can be divided into direct costs such as staff wages and consumable items, indirect costs such as building maintenance, leasing/mortgage payments and laundry services, professional fees such as anesthesia and surgeon fees, and specialty service fees such as intraoperative fluoroscopy, blood bank, lab, and orthopaedic implants. Most of these figures can be estimated from purchase orders and salaries payable by hospital accounting systems. More recently, time driven activity-based costing (TDABC) has allowed a more accurate way to assign cost in a complex environment where staff are often multi-tasking and thousands of consumables are utilized. TDABC divides complex care into discrete cycles allowing micro-costing assessment and assignment of cost based ontime. In either of these methods, decisions must be made when attempting to measure and/or conceptualize the actual cost of a surgery. It should be noted that data in the current literature pertaining to the cost of the operating room often, but not always, excludes the costs associated with anesthesia services, perioperative services, surgeon fees, blood bank expenses, radiology services, and implants. Consistent data on operating room costs is needed for effective healthcare resource allocation.”