da Silva JSV, et al. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr Clin Pract. 2020 Apr;35(2):178-195.

da Silva JSV, et al. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr Clin Pract. 2020 Apr;35(2):178-195.
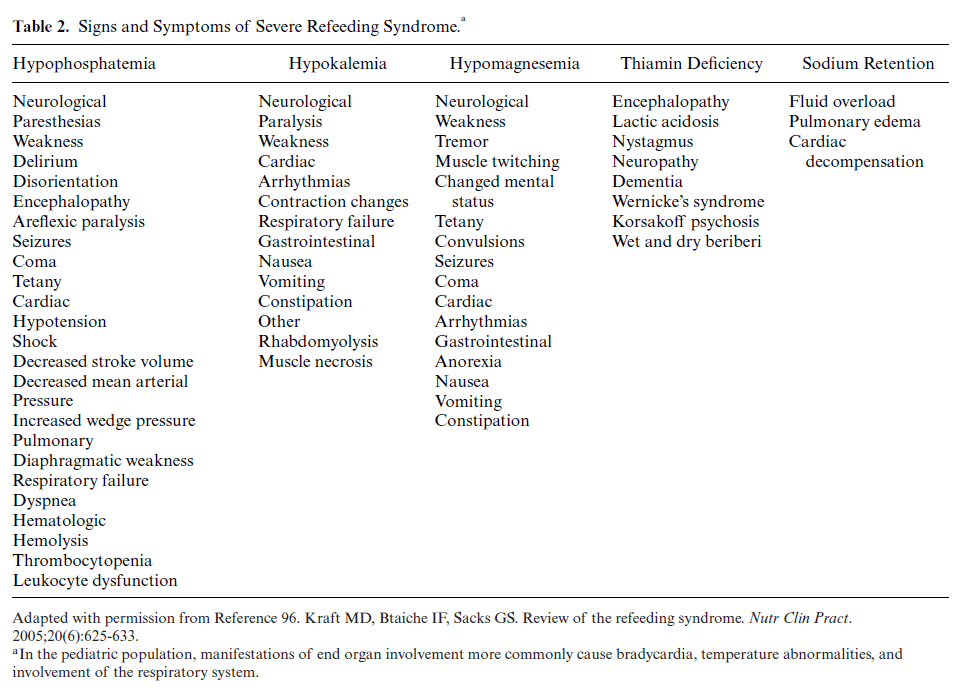
Madsen H, Frankel EH. The hitchhiker’s guide to parenteral nutrition management for adult patients. Practical Gastroenterology. 2006 Jul;30(7):46.
Summary: This was discussed as a possible question on boards. Below are three tables, taken directly from the article referenced.

Patel JJ, et al. Phase 3 Pilot Randomized Controlled Trial Comparing Early Trophic Enteral Nutrition With “No Enteral Nutrition” in Mechanically Ventilated Patients With Septic Shock. JPEN J Parenter Enteral Nutr. 2020 Jul;44(5):866-873.
Full-text for Emory users.
Results: One hundred thirty-one patients were eligible for enrollment, and 49 were available for consent. Thirty-one (86%) consented and were randomized and 100% of patients in the early EN arm and 94% in the “no EN” arm completed their protocols. While on vasopressors, early EN group received median 384 kcal, and the “no EN” group received median 0 kcal. Contamination rate was 0 in the early trophic EN arm and 6% in the “no EN” arm. The early EN group had median 25 intensive care unit-free days, as compared with 12 in the “no EN” arm (P = .014). The early EN arm had median 27 ventilator-free days, compared with 14 in “no EN” arm (P = .009).
Conclusion: Our protocol comparing early trophic EN with “no EN” in septic shock was feasible. Early trophic EN may be beneficial, but a larger multicenter trial is warranted to confirm the observed clinical benefits seen in this trial.
Kumpf VJ, et al. ASPEN-FELANPE Clinical Guidelines: Nutrition Support of Adult Patients With Enterocutaneous Fistula.JPEN J Parenter Enteral Nutr. 2017 Jan;41(1):104-112. doi: 10.1177/0148607116680792.
Questions addressed in these guidelines:
In adult patients with enterocutaneous fistula: (1) What factors best describe nutrition status? (2) What is the preferred route of nutrition therapy (oral diet, enteral nutrition, or parenteral nutrition)? (3) What protein and energy intake provide best clinical outcomes? (4) Is fistuloclysis associated with better outcomes than standard care? (5) Are immune-enhancing formulas associated with better outcomes than standard formulas?(6) Does the use of somatostatin or somatostatin analogue provide better outcomes than standard medical therapy? (7) When is home parenteral nutrition support indicated?
