“Because most patients die from progressive disease in the liver, hepatic arterial infusion pump (HAIP) chemotherapy with floxuridine is an attractive treatment option for unresectable [Intrahepatic cholangiocarcinoma] iCCA. The rationale for HAIP chemotherapy is that iCCA relies mostly on arterial blood supply. Moreover, floxuridine, also known as FUDR, is characterized by its high first-pass effect; approximately 95% is directly metabolized in the liver. Hence, this allows for an up to 400-fold dose increase in subsequent intratumoral exposure compared with systemic treatment, with minimal systemic exposure and side effects”
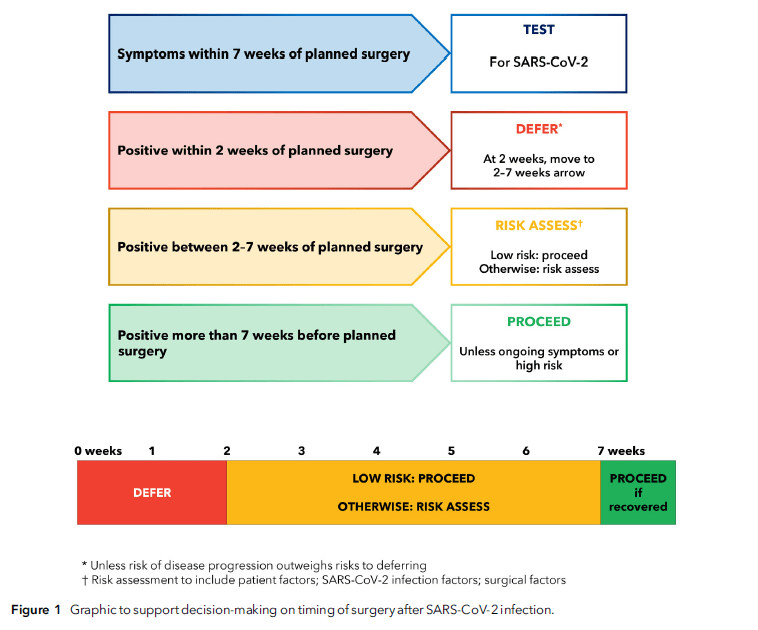
“Patients who develop symptoms of SARS-CoV-2 infection within 7 weeks of planned surgery, including on the day of surgery, should be screened for SARS-CoV-2. Elective surgery should not usually be undertaken within 2 weeks of diagnosis of SARS-CoV-2 infection. For patients who have recovered from SARS-CoV-2 infection and who are low risk or having low-risk surgery, most elective surgery can proceed 2 weeks following a SARS-CoV-2 positive test. For patients who are not low risk or having anything other than low-risk surgery between 2 and 7 weeks following infection, an individual risk assessment must be performed. This should consider: patient factors (age; comorbid and functional status); infection factors (severity; ongoing symptoms; vaccination); and surgical factors (clinical priority; risk of disease progression; grade of surgery).”
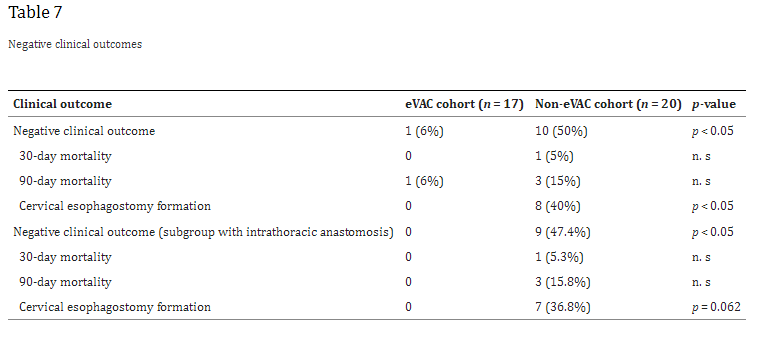
“Anastomotic leakages continue to be a highly challenging complication in esophageal surgery. According to the literature, the risk of anastomotic leakage after esophagectomy ranges between 4 and 35%. The location of the anastomotic leakage is a significant factor in determining patient outcomes. Notwithstanding, cervical anastomoses bear a higher risk for leakage; the consequences of an intrathoracic (mediastinal) leakage are usually more devastating. A leakage into the thoracic cavity typically leads to mediastinitis and severe pneumonia and contributes to the significant mortality rates in esophageal surgery. In contrast, cervical anastomotic leakages tend to frequently present as wound infections often only requiring external drainage”
“The clinical outcomes strongly depend on an early diagnosis and appropriate treatment, which can extent over several weeks or even months. In the past, the mainstay of treatment was based on surgical repair, external drainage of sepsis via chest tubes, and interventional treatment modalities like endoscopic stent deployment or clipping. In 2008, endoscopic vacuum-assisted closure (eVAC) therapy was successfully applied in patients with anastomotic leakages after esophagectomies. As in other vacuum-assisted wound therapies, eVAC cleans the defect by reducing the amount of exudative fluids and necrotic tissue, thus accelerating the healing process by contributing to a better local perfusion as well as through the formation of granulation tissue.”
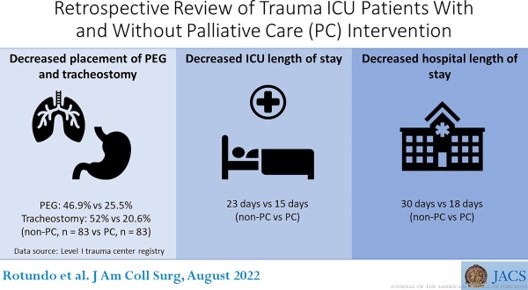
“Older trauma patients present with poor preinjury functional status and more comorbidities. Advances in care have increased the chance of survival from previously fatal injuries with many left debilitated with chronic critical illness and severe disability. Palliative care (PC) is ideally suited to address the goals of care and symptom management in this critically ill population. A retrospective chart review was done to identify the impact of PC consults on hospital length of stay (LOS), ICU LOS, and surgical decisions.”
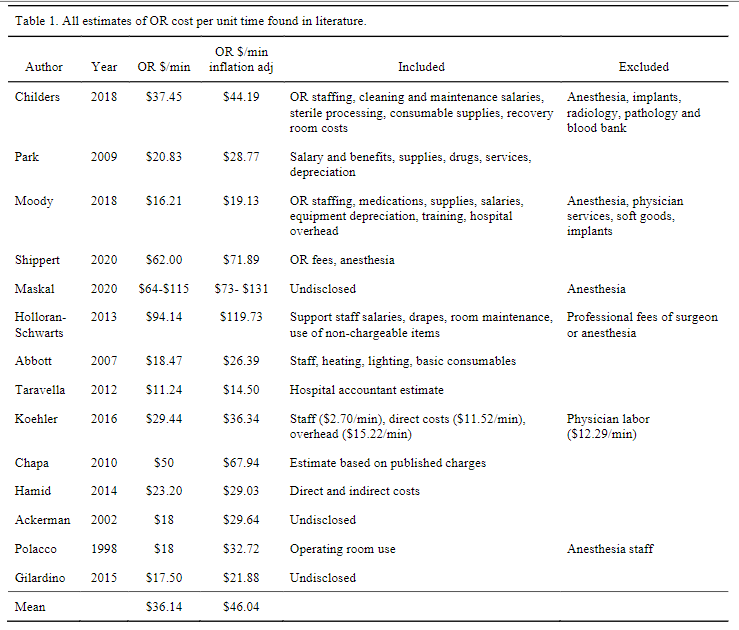
“The cost to run an operating room can be divided into direct costs such as staff wages and consumable items, indirect costs such as building maintenance, leasing/mortgage payments and laundry services, professional fees such as anesthesia and surgeon fees, and specialty service fees such as intraoperative fluoroscopy, blood bank, lab, and orthopaedic implants. Most of these figures can be estimated from purchase orders and salaries payable by hospital accounting systems. More recently, time driven activity-based costing (TDABC) has allowed a more accurate way to assign cost in a complex environment where staff are often multi-tasking and thousands of consumables are utilized. TDABC divides complex care into discrete cycles allowing micro-costing assessment and assignment of cost based ontime. In either of these methods, decisions must be made when attempting to measure and/or conceptualize the actual cost of a surgery. It should be noted that data in the current literature pertaining to the cost of the operating room often, but not always, excludes the costs associated with anesthesia services, perioperative services, surgeon fees, blood bank expenses, radiology services, and implants. Consistent data on operating room costs is needed for effective healthcare resource allocation.”