“Pancreas-sparing duodenectomy, although technically demanding, eliminates the need for pancreatic resection. Pancreas-sparing duodenectomy is associated with good absorptive capacity, weight gain, and quality of life. Furthermore, it may reduce the risk of subsequent malignancy. Long-term surveillance, however, is still required. Pancreas-sparing duodenectomy is contraindicated in the setting of malignancy.”
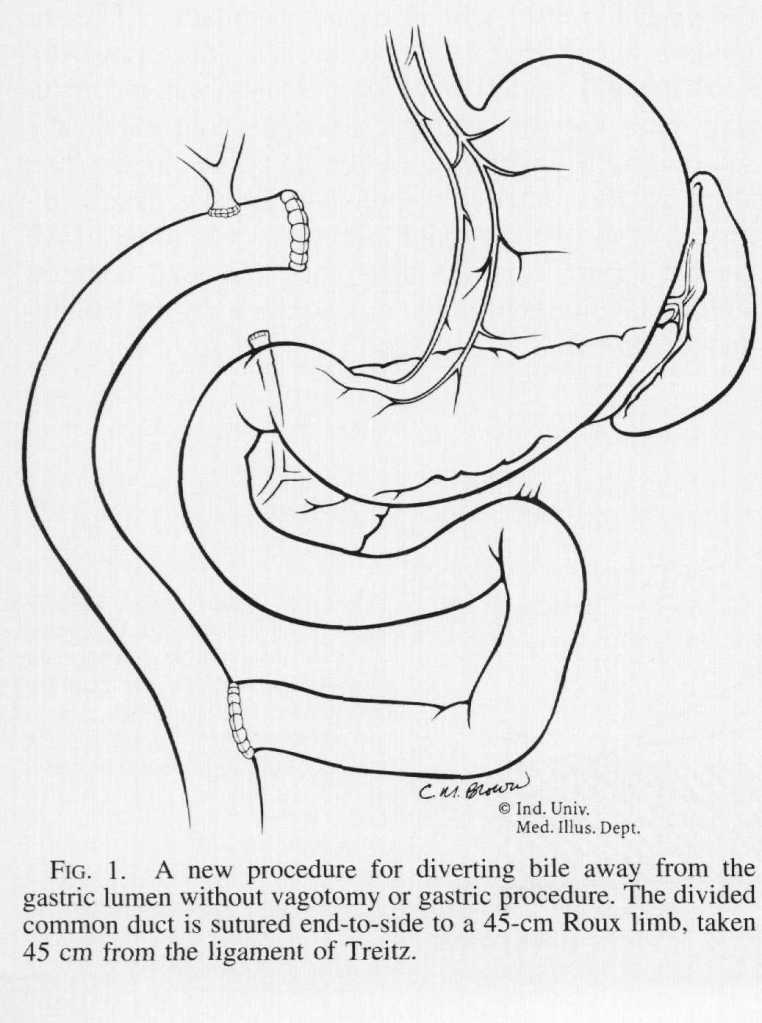
“Various treatments for [Primary Bile Reflux Gastritis] have been proposed since its recognition. Operations that have been utilized are the Roux-en-Y procedure, the Braun enteroenterostomy, the Henley jejunal interposition, and several modifications of each of these operations. These procedures produce relief from bile reflux, but all have particular side effects of their own. Before the utilization of vagotomy for ulcer disease, stomal ulceration at the gastrojejunal anastomosis was the most frequent postoperative problem. Currently, the most commonly applied operation is the Roux-en-Y gastrojejunostomy, which requires vagotomy and antrectomy and results in the equally disabling Roux stasis syndrome in about one-half of patients.”
“Because of these difficulties, a new procedure is proposed wherein only bile is diverted by means of a Roux-en-Y limb and no gastric procedure is done. This allows minimal disturbance of gastric motility and totally diverts bile away from the gastric lumen.”
“Because most patients die from progressive disease in the liver, hepatic arterial infusion pump (HAIP) chemotherapy with floxuridine is an attractive treatment option for unresectable [Intrahepatic cholangiocarcinoma] iCCA. The rationale for HAIP chemotherapy is that iCCA relies mostly on arterial blood supply. Moreover, floxuridine, also known as FUDR, is characterized by its high first-pass effect; approximately 95% is directly metabolized in the liver. Hence, this allows for an up to 400-fold dose increase in subsequent intratumoral exposure compared with systemic treatment, with minimal systemic exposure and side effects”
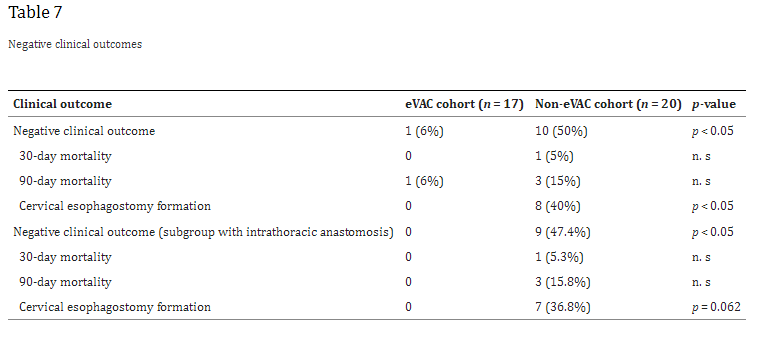
“Anastomotic leakages continue to be a highly challenging complication in esophageal surgery. According to the literature, the risk of anastomotic leakage after esophagectomy ranges between 4 and 35%. The location of the anastomotic leakage is a significant factor in determining patient outcomes. Notwithstanding, cervical anastomoses bear a higher risk for leakage; the consequences of an intrathoracic (mediastinal) leakage are usually more devastating. A leakage into the thoracic cavity typically leads to mediastinitis and severe pneumonia and contributes to the significant mortality rates in esophageal surgery. In contrast, cervical anastomotic leakages tend to frequently present as wound infections often only requiring external drainage”
“The clinical outcomes strongly depend on an early diagnosis and appropriate treatment, which can extent over several weeks or even months. In the past, the mainstay of treatment was based on surgical repair, external drainage of sepsis via chest tubes, and interventional treatment modalities like endoscopic stent deployment or clipping. In 2008, endoscopic vacuum-assisted closure (eVAC) therapy was successfully applied in patients with anastomotic leakages after esophagectomies. As in other vacuum-assisted wound therapies, eVAC cleans the defect by reducing the amount of exudative fluids and necrotic tissue, thus accelerating the healing process by contributing to a better local perfusion as well as through the formation of granulation tissue.”
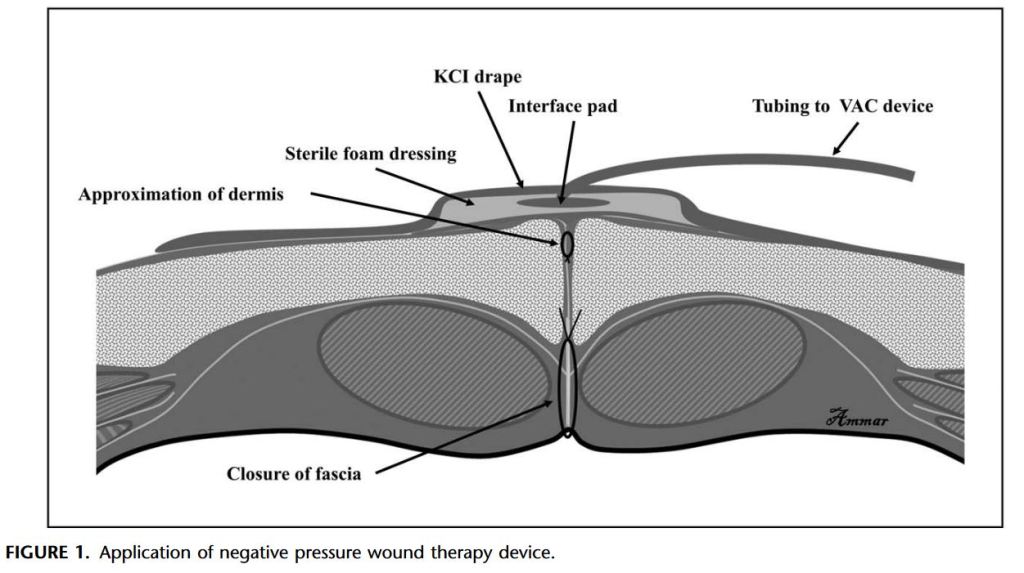
“Despite improvement in infection control, SSIs remain a common cause of morbidity after abdominal surgery. SSI has been associated with an increased risk of reoperation, prolonged hospitalization, readmission, and higher costs. Recent retrospective studies have suggested that the use of negative pressure wound therapy can potentially prevent this complication.”
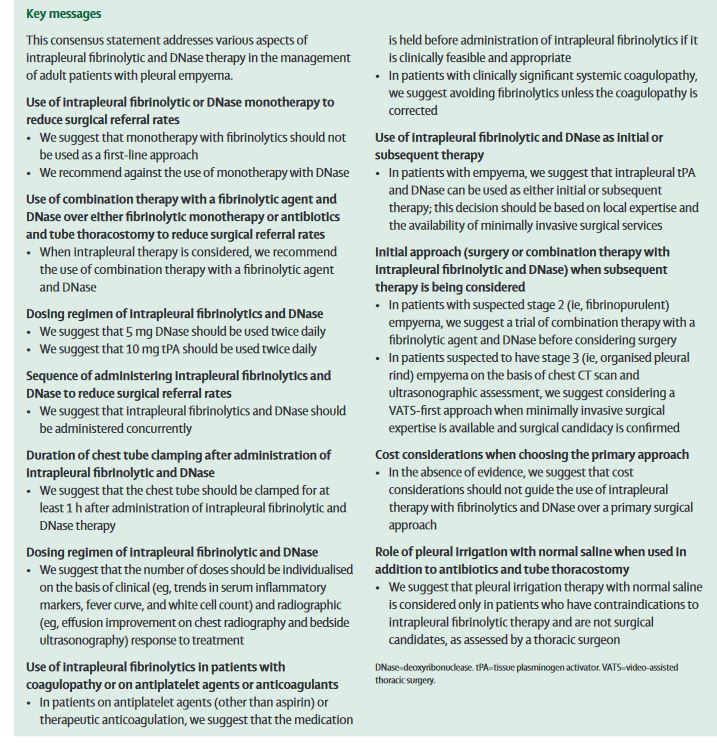
“Parapneumonic effusions evolve through a spectrum of three stages. The initial exudative stage (stage 1; analogous to simple parapneumonic effusion) is characterised by an increased outpouring of fluid into the pleural space mediated by capillary permeability. If left untreated, persistent inflammation with the associated rise in fluid plasminogen activator inhibitor causes a decrease in fluid fibrinolytic concentrations. During this second stage (stage 2; fibrinopurulent stage), as the effusion becomes infected, septations and adhesions induced by fibrin deposition divide the space into pockets or locules. With the proliferation of fibroblasts and the formation of a pleural peel, lung expansion becomes restricted and can result in a non-expandable lung. It is important to initiate all medical treatment before this final so-called organising stage (stage 3) ensues.”
“Empyema thoracis, from the Greek, is defined as ‘‘pus in the chest.’’ The most common precursor of empyema is bacterial pneumonia and subsequent parapneumonic effusion. Other causes of empyema include bronchogenic carcinoma, esophageal rupture, blunt or penetrating chest trauma, mediastinitis with pleural extension, infected congenital cysts of the airway and esophagus, extension from sources below the diaphragm, cervical and thoracic spine infections, as well as postsurgical etiologies.”