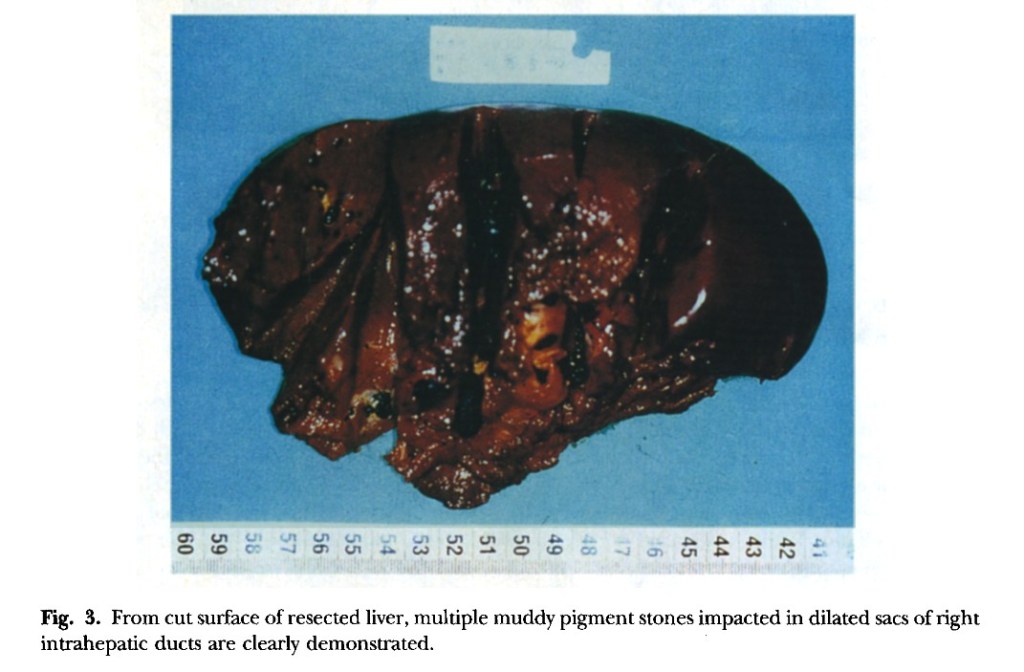
“Hepatic resection has been thought to he the most effective treatment modality for selected patients who have left-sided hepatolithiasis and meet the criteria of resection.” Under the same criteria the role of right hepatic resection, especially right hepatic lobectomy, is still ambiguous for patients who have right-sided hepatolithiasis because of the higher operative risk. This report presents the results of right hepatic lobectomy in the treatment of patients with right-sided hepatolithiasis after careful selection. In particular, we focus on the
rationale and indications for this procedure,”