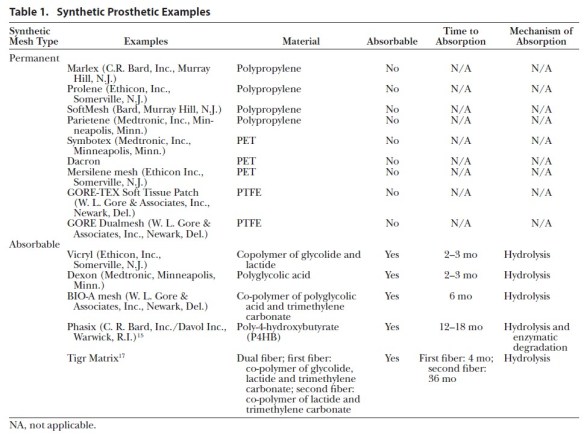
Lak KL, Goldblatt MI. Mesh Selection in Abdominal Wall Reconstruction. Plast Reconstr Surg. 2018 Sep;142(3 Suppl):99S-106S. Full-text for Emory users.

Lak KL, Goldblatt MI. Mesh Selection in Abdominal Wall Reconstruction. Plast Reconstr Surg. 2018 Sep;142(3 Suppl):99S-106S. Full-text for Emory users.
Rechenmacher SJ, Fang JC. Bridging Anticoagulation: Primum Non Nocere. J Am Coll Cardiol. 2015 Sep 22;66(12):1392-403.
Full-text for Emory users.
Conclusions: Periprocedural anticoagulation management is a common clinical dilemma with limited evidence (but 1 notable randomized trial) to guide our practices. Although bridging anticoagulation may be necessary for those patients at highest risk for TE, for most patients it produces excessive bleeding, longer length of hospital stay, and other significant morbidities, while providing no clear prevention of TE. Unfortunately, contemporary clinical practice, as noted in physician surveys, continues to favor interruption of OAC and the use of bridging anticoagulation. While awaiting the results of additional randomized trials, physicians should carefully reconsider the practice of routine bridging and whether periprocedural anticoagulation interruption is even necessary.
 Central Illustration. Bridging Anticoagulation: Algorithms for Periprocedural Interrupting and Bridging Anticoagulation. Decision trees for periprocedural interruption of chronic oral anticoagulation (top) and for periprocedural bridging anticoagulation (bottom). OAC = oral anticoagulation.
Central Illustration. Bridging Anticoagulation: Algorithms for Periprocedural Interrupting and Bridging Anticoagulation. Decision trees for periprocedural interruption of chronic oral anticoagulation (top) and for periprocedural bridging anticoagulation (bottom). OAC = oral anticoagulation.
Nandipati KC, Lin E, Husain F, Srinivasan J, Sweeney JF, Davis SS. Counterclockwise rotation of Roux-en-Y limb significantly reduces internal herniation in laparoscopic Roux-en-Y gastric bypass (LRYGB). J Gastrointest Surg. 2012 Apr;16(4):675-81.
Full-text for Emory users.
Continue readingNicolson NG, Han D. Desmoplastic melanoma. J Surg Oncol. 2019 Jan;119(2):208-215. doi: 10.1002/jso.25317. Epub 2018 Nov 27.
Desmoplastic melanoma (DM) is a rare melanoma variant that has unique biology and pathology compared with conventional melanoma (non-DM). Importantly, DM is classified into pure and mixed histologic subtypes, which have been correlated with outcomes. Management of DM broadly mirrors that of non-DM; however, there are unique considerations for DM that influence treatment approaches. This paper will provide a contemporary overview of this disease and will review the literature regarding the management of DM.
Continue reading| Emory users, open this instance of PubMed, then click the links below for full-text article access. |
Anal fistulas
Sugrue J, et al. Sphincter-Sparing Anal Fistula Repair: Are We Getting Better? Dis Colon Rectum. 2017 Oct;60(10):1071-1077. doi: 10.1097/DCR.0000000000000885.
Vogel JD, et al. Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula Dis Colon Rectum. 2016 Dec;59(12):1117-1133. doi: 10.1097/DCR.0000000000000733.
Sirany AM, et al. The ligation of the intersphincteric fistula tract procedure for anal fistula: a mixed bag of results Dis Colon Rectum. 2015 Jun;58(6):604-12. doi: 10.1097/DCR.0000000000000374.
Diverticulitis:
Francis NK, et al. EAES and SAGES 2018 consensus conference on acute diverticulitis management: evidence-based recommendations for clinical practice Surg Endosc. 2019 Sep;33(9):2726-2741. doi: 10.1007/s00464-019-06882-z.
Fissures
Murad-Regadas SM, et al. How much of the internal sphincter may be divided during lateral sphincterotomy for chronic anal fissure in women? Morphologic and functional evaluation after sphincterotomy Dis Colon Rectum. 2013 May;56(5):645-51. doi: 10.1097/DCR.0b013e31827a7416.
Stewart DB Sr, et al. Clinical Practice Guideline for the Management of Anal Fissures Dis Colon Rectum. 2017 Jan;60(1):7-14. doi: 10.1097/DCR.0000000000000735.
Thornton MJ, et al. Prospective manometric assessment of botulinum toxin and its correlation with healing of chronic anal fissure Dis Colon Rectum. 2005 Jul;48(7):1424-31. doi: 10.1007/s10350-005-0025-9.
Hemorrhoids
Davis BR, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids Dis Colon Rectum. 2018 Mar;61(3):284-292. doi: 10.1097/DCR.0000000000001030.
Nelson DW, et al. Prophylactic antibiotics for hemorrhoidectomy: are they really needed? Dis Colon Rectum. 2014 Mar;57(3):365-9. doi: 10.1097/DCR.0b013e3182a0e522.
Nienhuijs S, et al. Conventional versus LigaSure hemorrhoidectomy for patients with symptomatic Hemorrhoids Cochrane Database Syst Rev. 2009 Jan 21;2009(1):CD006761. doi: 10.1002/14651858.CD006761.pub2.
Rectal prolapse
Bordeianou L, et al. Clinical Practice Guidelines for the Treatment of Rectal Prolapse Dis Colon Rectum. 2017 Nov;60(11):1121-1131. doi: 10.1097/DCR.0000000000000889.
Colon cancer
Allaix ME, Rebecchi F, Fichera A. The Landmark Series: Minimally Invasive (Laparoscopic and Robotic) Colorectal Cancer Surgery. Ann Surg Oncol. 2020 Oct;27(10):3704-3715.
Alonso S, Saltz L. The Landmark Series: Chemotherapy for Non-Metastatic Colon Cancer. Ann Surg Oncol. 2021 Feb;28(2):995-1001.
_________________________________________________________________________
Pneumatosis Intestinalis:
Sanford Z, et al Updates on the Utility of Diagnostic Laparoscopy in the Management of Pneumatosis Intestinalis: An Improvement to the Current Treatment Algorithm. Surg Innov. 2018 Dec;25(6):648-650.
Rectal Cancer
Peacock O, Chang GJ. The Landmark Series: Management of Lateral Lymph Nodes in Locally Advanced Rectal Cancer. Ann Surg Oncol. 2020 Aug;27(8):2723-2731.
Bahadoer RR, Dijkstra EA, van Etten B, et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021 Jan;22(1):29-42. doi: 10.1016/S1470-2045(20)30555-6. Epub 2020 Dec 7. Erratum in: Lancet Oncol. 2021 Feb;22(2):e42. PMID: 33301740.
Conroy T, Lamfichekh N, Etienne P, Rio E, Francois E, Mesgouez-Nebout N, et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: final results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J Clin Oncol 2020;38(15 Suppl.):4007.
Ferrara M, Kann BR. Urological injuries during colorectal surgery. Clin Colon Rectal Surg. 2019 May;32(3):196-203.
“A recent retrospective population-based study of patients in the United States undergoing colorectal surgery found the overall incidence of ureteral injury to be 0.28%. The incidence was found to be significantly higher in patients with stage 3 or 4 cancer, malnutrition, steroid use, and in operations done at teaching hospitals. Rectal cancer cases were found to have the highest rates of ureteral injuries (7.1/1,000), followed by Crohn’s disease and diverticular disease (2.9/1,000 each). In this review, laparoscopic surgery was associated with a lower incidence of ureteral injuries when compared with open (1.1 vs. 2.8/1,000, p < 0.001). Of the specific operations reviewed, abdominoperineal resection (APR) was found to have the highest rate of ureteral injury at 7.1/1,000 cases.” (Ferrara, 2019, p. 196)
Continue readingWe are excited to share a new section titled “Essential Articles for Surgical Residents.”
Keeping up with surgical literature in residency can be challenging. This list was created to serve as an easily accessible, up-to-date, and evidence-based resource for residents.
The content has been curated by faculty from each department and is intended to supplement the standard educational curriculum of each rotation with current and relevant literature.
Continue reading