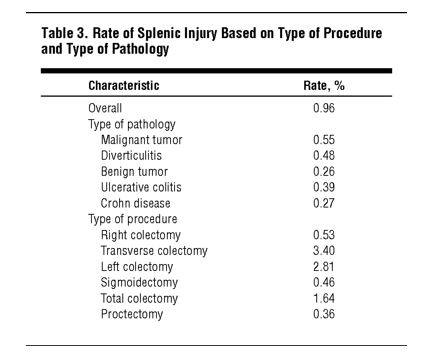
“Splenic injury is a major intraoperative complication of abdominal surgery and places patients at a higher risk of morbidity and mortality, of longer operating time, and of longer hospital stay. Splenic injuries may be managed nonoperatively or by splenorrhaphy, partial splenectomy, or complete splenectomy. Because splenectomy is reported to have higher mortality rates than splenorrhaphy, great effort is taken to preserve the spleen; however, excessive blood loss can mandate splenectomy.”
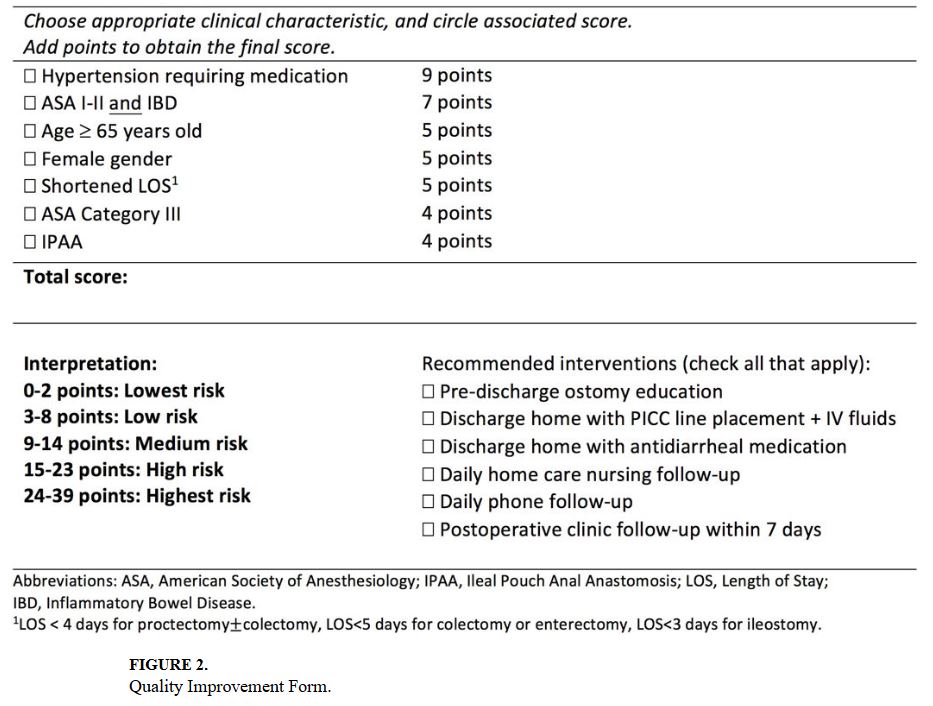
“Readmission within 30-days of hospital discharge has received widespread attention as a potential healthcare quality indicator. In 2013, the Center for Medicare and Medicaid Services established the Hospital Readmission Reduction Program (HRRP), a cost- containment strategy that financially penalizes hospitals with higher than expected 30-day readmission. Though conditions targeted by the HRRP have been predominately medical, it is anticipated that readmission after surgical procedures will be used to structure financial incentives and hospital compensation in the near future.”
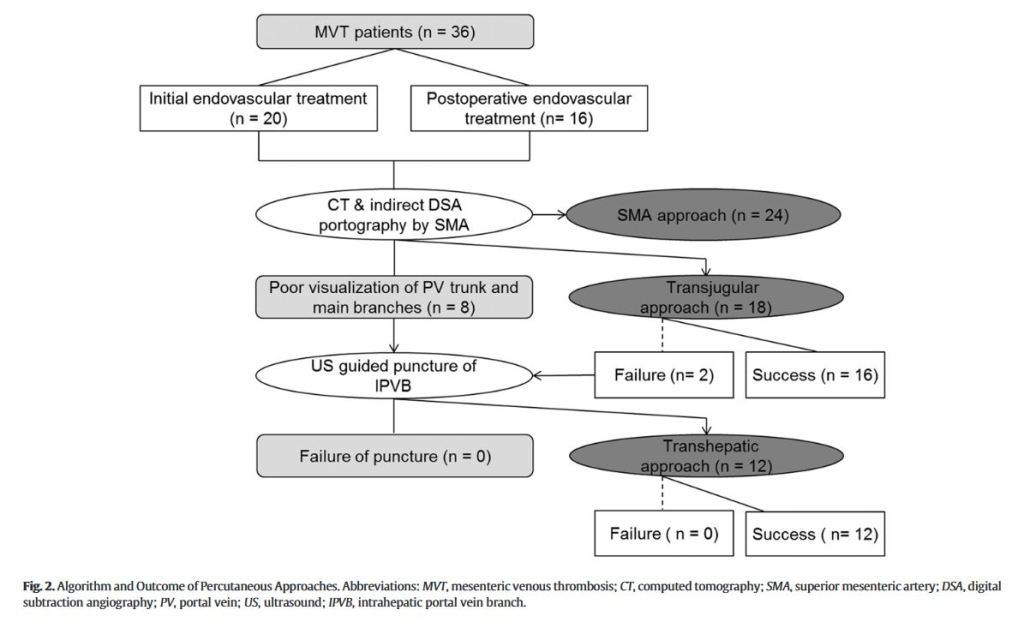
“Acute mesenteric ischemia (AMI) is a rare but catastrophic abdominal vascular emergency associated with a daunting mortality comparable to myocardial infarction or cerebral stroke. Mesenteric vein thrombosis (MVT) is the least common form, accounting for 6% to 9%, of AMI, mainly involving the superior mesenteric vein (SMV). Despite the lack of specific biomarker and insidious symptomatology profile, incidence of acute superior mesenteric venous thrombosis (ASMVT) has been increasing worldwide due to the raised awareness as well as widespread use of contrast-enhanced computed tomography (CT) portography, which facilitates early diagnosis with sensitivity of over 90%.”
“Patients and families who are language discordant with their clinical teams report lower patient satisfaction, worse health status, and lower rates of having a regular healthcare provider and obtaining preventive care services. When patients and parents with a non-dominant language preference access care, they report difficulty communicating and understanding medical information from providers, comprehending written medical information, reading prescription bottles, and accessing interpretation services. Individuals with non-dominant language preferences have also been shown to experience more medical errors and adverse health events.”
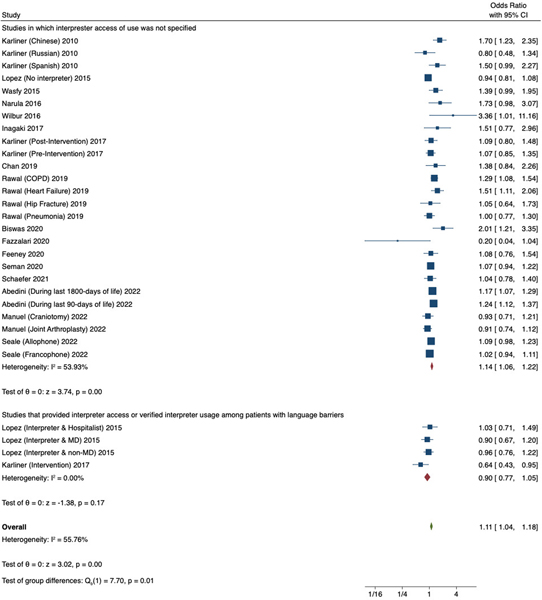
Figure 2. Meta-analysis of studies that evaluated differences in 28-day or 30-day hospital readmission rate among adult patients with versus without a dominant langauge preference, stratified by studies that provided interpreter access or verified interpreter usage among patients with non-dominant language preference versus studies in which interpreter access or use was not specified. COPD, chronic obstructive pulmonary disease.Continue reading →
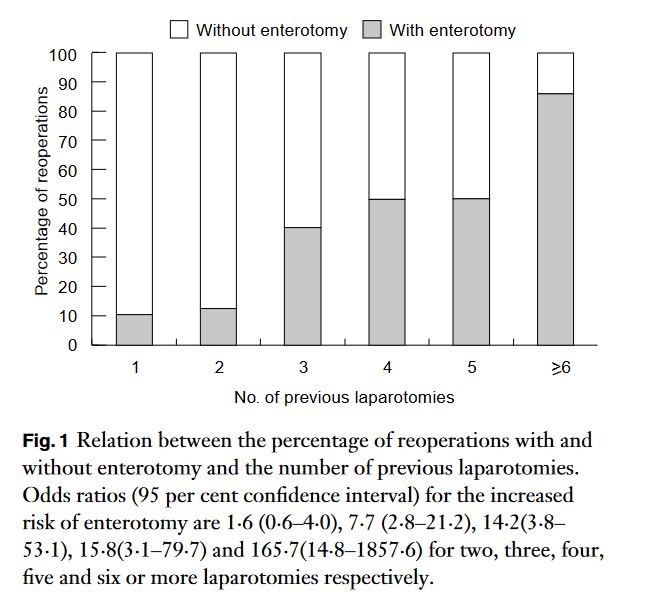
“Postoperative intra-abdominal adhesions are a major concern in modern surgery. Intestinal obstruction is an important and well known clinical consequence of adhesions, resulting in significant morbidity and mortality rates, and high financial costs. Secondary infertility in women and chronic abdominal and pelvic pain are other, frequently cited, adhesion-related problems. Furthermore, intraabdominal adhesions render reoperation dif®cult and may increase the complication rate of the intended surgical procedure. Prolonged operating time, unfeasibility of the laparoscopic approach and inadvertent enterotomy are known drawbacks of reoperative abdominal surgery, directly related to adhesions.”
“The refusal of blood transfusion for surgical procedures at high risk of bleeding, such as pancreatic resection, forces surgeons to face ethical challenges and raises concerns about appropriate perioperative management. In the last two decade the rate of transfusion in high volume centers has gradually decreased thanks to the application of patient blood management (PBM) protocols.”
“In our single-institution experience, patients that categorically refused transfusion were Jehovah’s Witnesses (JW). JW is a religious movement, membership in which accounts for about 0.3% of Western countries’ populations, with USA and Italy having the highest percentages of followers. JW followers believe neither whole blood nor its four major components, namely red cells, white cells, platelets and plasma, should be donated, stored, or accepted in any circumstance, even in life-threatening situations. Advances in transfusion medicine have led the JW’s denomination to modify its position about what is deemed acceptable.”
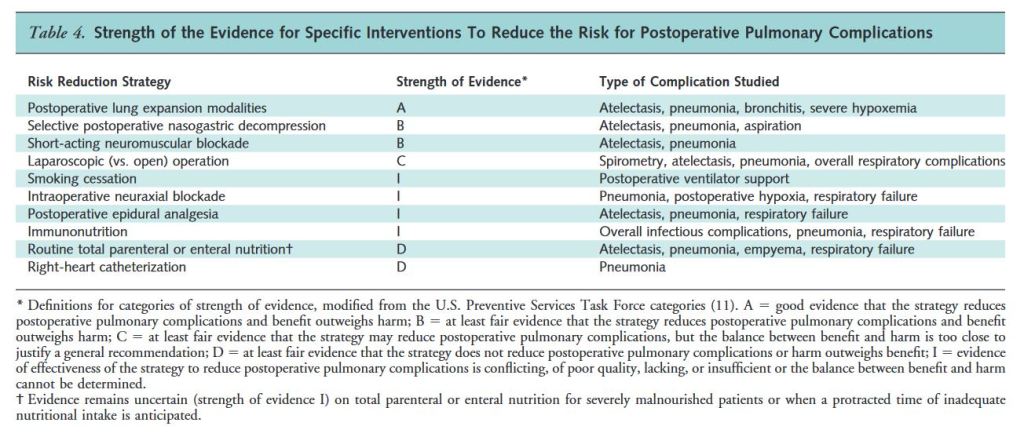
“Postoperative pulmonary complications are as common as cardiac complications for patients undergoing non-cardiothoracic surgery. Further, these complications have similar mortality rates and length of stay after elective abdominal surgery or hip fracture repair. This current systematic review synthesizes the evidence on preventive strategies and focuses on atelectasis, pneumonia, and respiratory failure.”