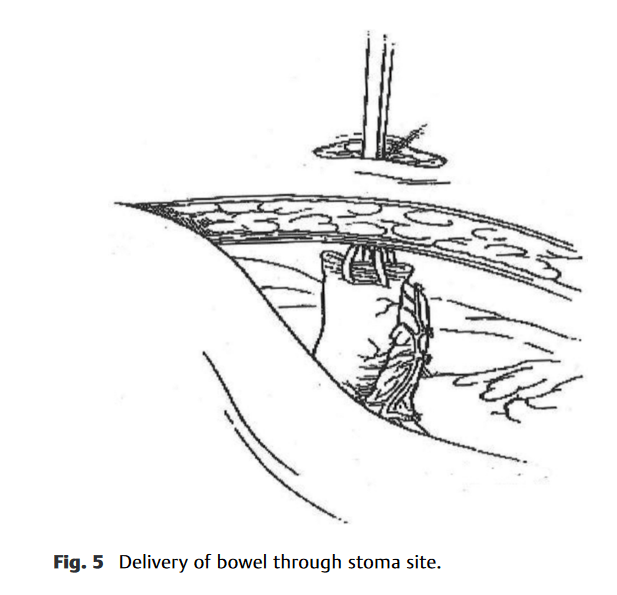
“Intestinal stomas are the surgical exteriorization of either small or large bowel through the anterior abdominal wall. While the principles behind stoma creation are typically the same, there are many different stoma configurations that are created for myriad indications.”
“Although the American Heart Association (AHA) and American College of Cardiology (ACC) and the American College of Chest Physicians (ACCP) provide guidelines on anticoagulation for patients with MHVs, limited guidance is provided for bridging anticoagulation 2,3 The guidelines are focused on preoperative bridging, with virtually no guidance on postoperative bridging.”
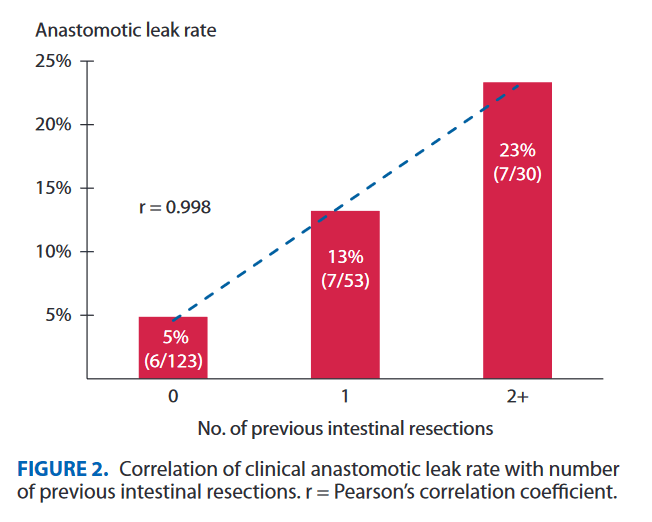
“Repeat intestinal resection in patients with Crohn’s disease is associated with an increased rate of anastomotic leakage when compared with initial resection despite similar patient, medication, and procedural factors.”
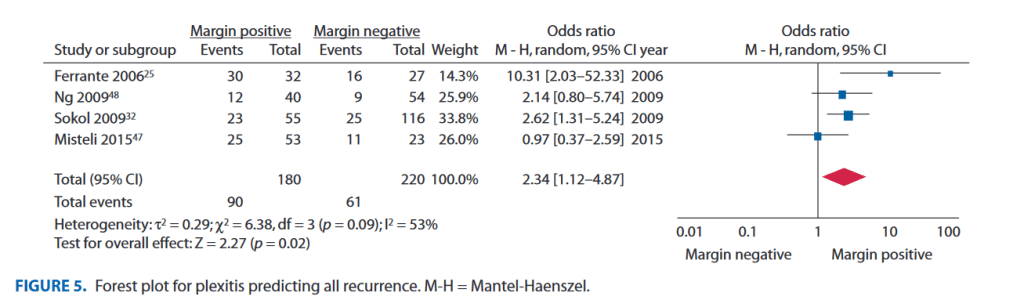
“The presence of involved histological margins at the time of index resection in Crohn’s disease is associated with recurrence, and plexitis shows promiseas a marker of more aggressive disease. Further studies with homogeneity of histopathological and recurrence reporting are required.“”The presence of involved histological margins at the time of index resection in Crohn’s disease is associated with recurrence, and plexitis shows promiseas a marker of more aggressive disease. Further studies with homogeneity of histopathological and recurrence reporting are required.“
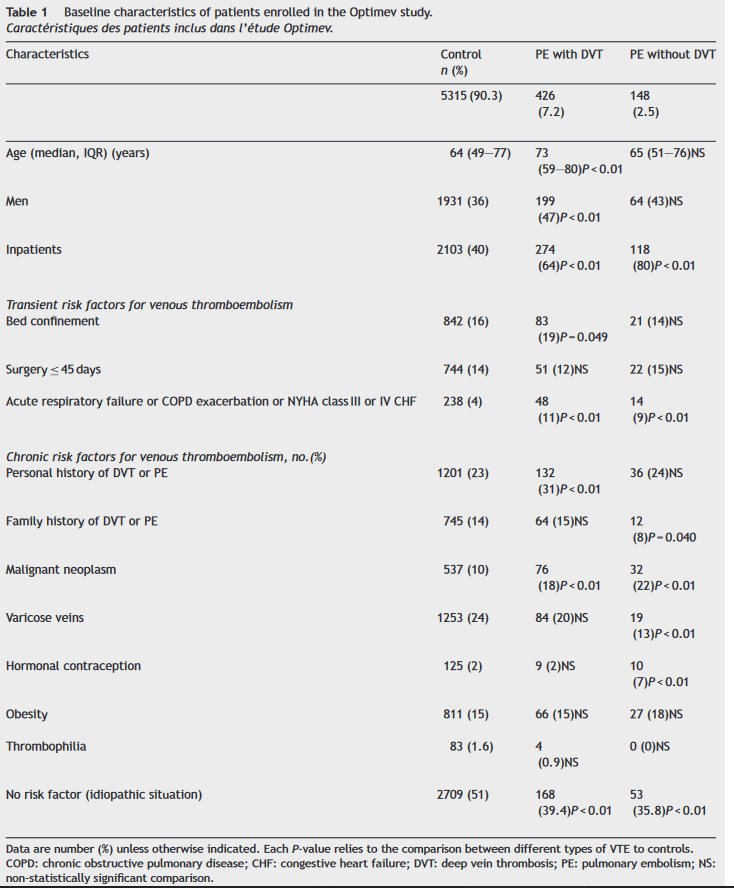
“Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common clinical problem associated with significant mortality and life-long morbidity among hospitalized patients and outpatients. The diagnosis of VTE is challenging because of the non specific signs and symptoms of this disease.”
“The aim of this study was to investigate the clinical presentation and 3-month mortality associated with some forms of VTE: PE with DVT, and PE without DVT.”
“Anaphylaxis is described as a severe, life‑threatening, generalized or systemic hypersensitivity reaction. It occurs rarely during surgery and anesthesia but neuromuscular blocking agents, non‑steroidal anti‑inflammatory drugs (NSAIDs), and antibiotics are considered common causes of anaphylaxis”
“Sugammadex is a synthetic modified gamma‑cyclodextrin derivative first designed to selectively bind to the steroidal neuromuscular blocking agent molecule to provide rapid recovery of neuromuscular function. Sugammadex is extensively used for reversing the effects of rocuronium and to a lesser extent, vecuronium.”
The most commonly involved agents in perioperative anaphylaxis are NMBAs, antibiotics, antiseptics, latex, and dyes However, any medication or substance the patient comes into contact with perioperatively can be a potential cause. The primary risk factor is a previous perioperative anaphylaxis or allergy to the medications or substances used in the procedure.