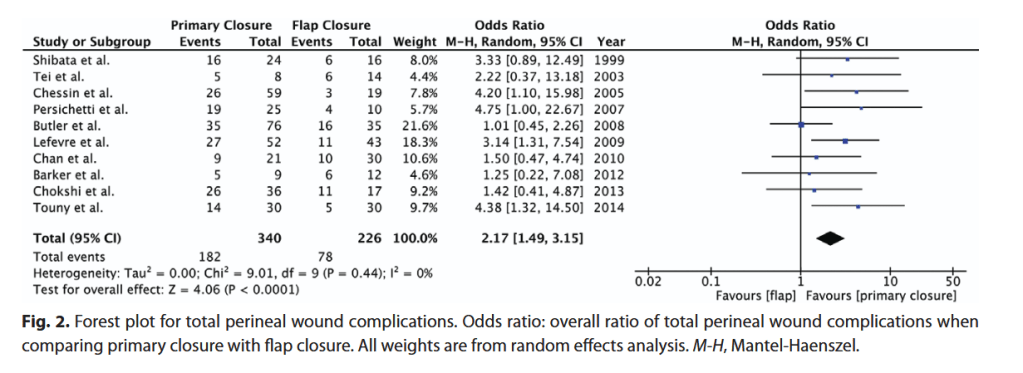
“Abdominoperineal resection and pelvic exenteration for resection of malignancies can lead to large perineal defects with significant surgical-site morbidity. Myocutaneous flaps have been proposed in place of primary closure to improve wound healing. A systematic review was conducted to compare primary closure with myocutaneous flap reconstruction of perineal defects following abdominoperineal resection or pelvic exenteration with regard to
surgical-site complications.”