“Distal pancreatectomy with splenectomy (DPS) is performed to remove pathology of the body and/or tail of the pancreas. The spleen and the left side of the pancreas share blood supply, and often tumor involvement, thus splenectomy is often performed along with distal
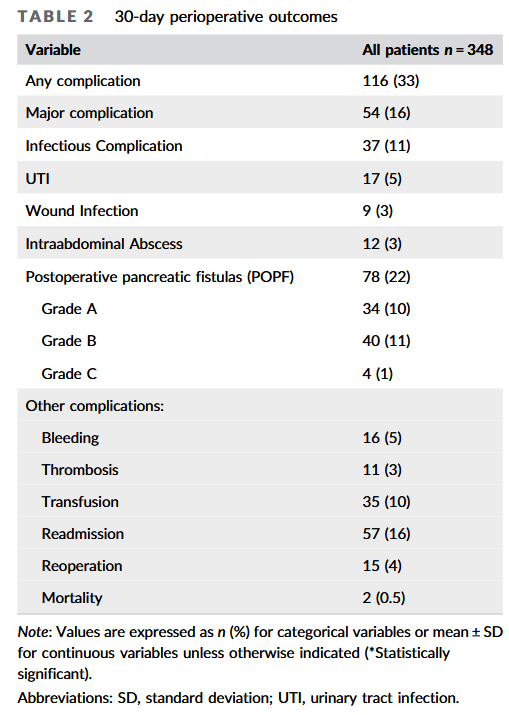
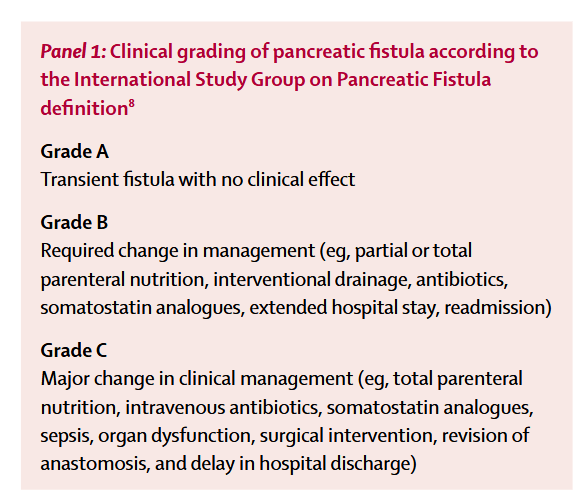
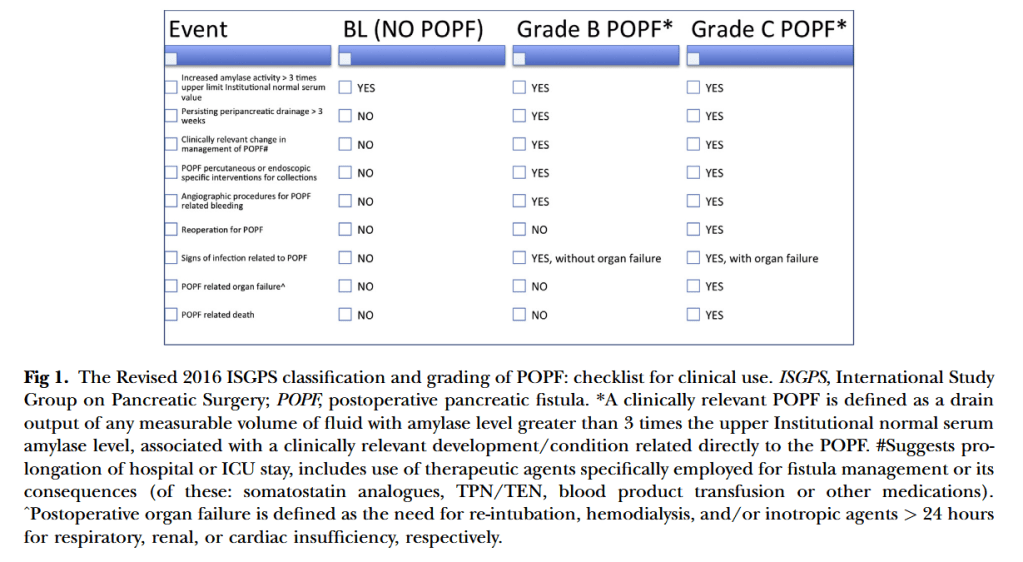
pancreatectomy. DPS is an operation that carries a greater than 30% risk of postoperative complications, including infection, postoperative pancreatic fistula (POPF), intraabdominal abscesses, and pneumonia, among others. In addition to these immediate postoperative
complications, splenectomy itself is known to confer long‐term susceptibility to infection, sepsis, thrombosis, and other sequelae. Our goal was to identify factors that could prompt early investigation and treatment of both infectious and major complications.”