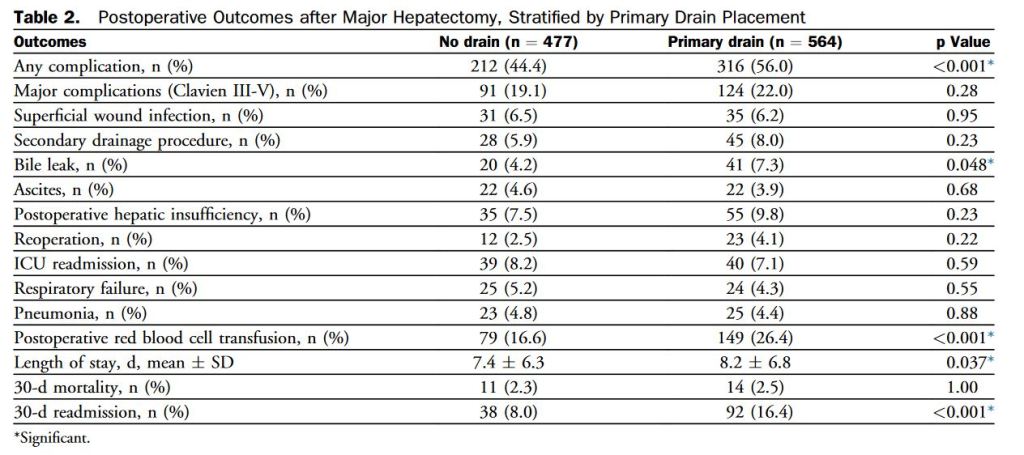
“Historically, prophylactic intraoperative peritoneal drain placement has been advocated after hepatectomy in order to identify and drain bile leaks and decrease the risk of potential perihepatic fluid collections and abscess formation postoperatively. Several small randomized trials have suggested, however, that routine abdominal drainage after elective liver resection may not be necessary.”