Abstract
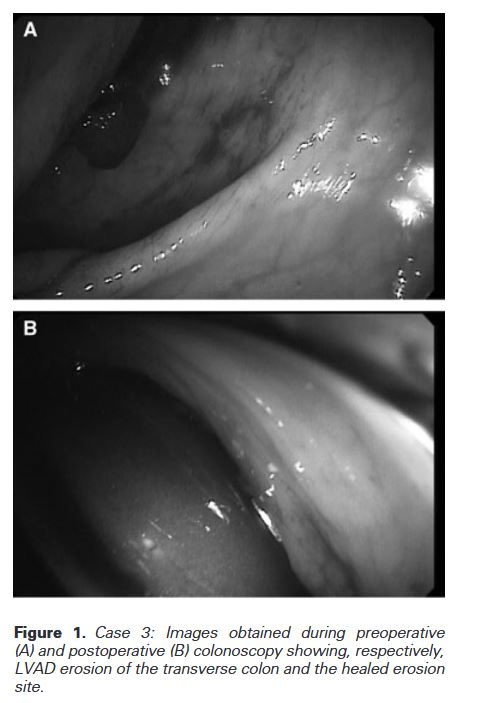
“A man in his early 20s with heart failure with reduced ejection fraction secondary to non-compaction cardiomyopathy (Titin (TTN) gene mutation positive) was transitioned from left ventricular assist device (LVAD) mechanical support to heart transplantation. Transplantation was successful; however, LVAD explantation resulted in innumerable complications secondary to penetration of the driveline into the peritoneal cavity. He developed an enterocutaneous fistula which led to concurrent malnutrition, poor wound healing, systemic infection, and allograft rejection in a patient less than 1 month after heart transplantation on immunosuppression.”
Tan, Derek W et al. “Enterocutaneous fistula formation after cardiac transplantation due to injury from LVAD driveline migration.” BMJ case reports vol. 16,6 e254696. 22 Jun. 2023 Emory Users Request Article via Interlibrary Loan