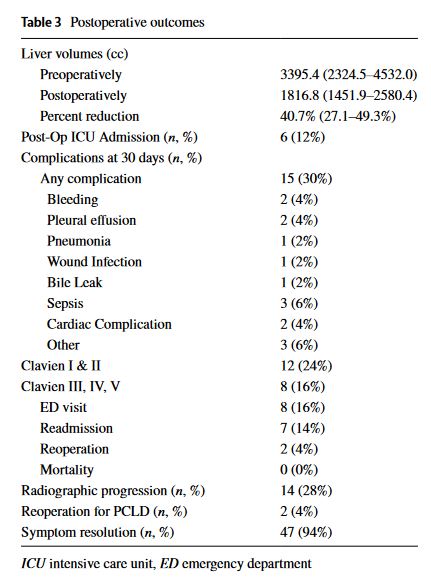
“Given the relative rarity of PCLD, current data on the outcomes of surgical debulking for advanced PCLD are scarce, particularly within the realm of laparoscopic hepatic resection techniques. We therefore sought to evaluate the characteristics of patients undergoing operative debulking for advanced PCLD and analyze the perioperative and long- term postoperative outcomes of hepatic resection for PCLD.”
“Adult polycystic liver disease (PCLD) is an autosomal dominant condition commonly associated with autosomal dominant polycystic kidney disease (ADPKD). However in the last decade, it has been recognized that there is a distinct form of autosomal dominant PCLD that arises without concomitant ADPKD. Early knowledge of the pathogenesis was gained from the study of hepatic cysts in patients with ADPKD.”
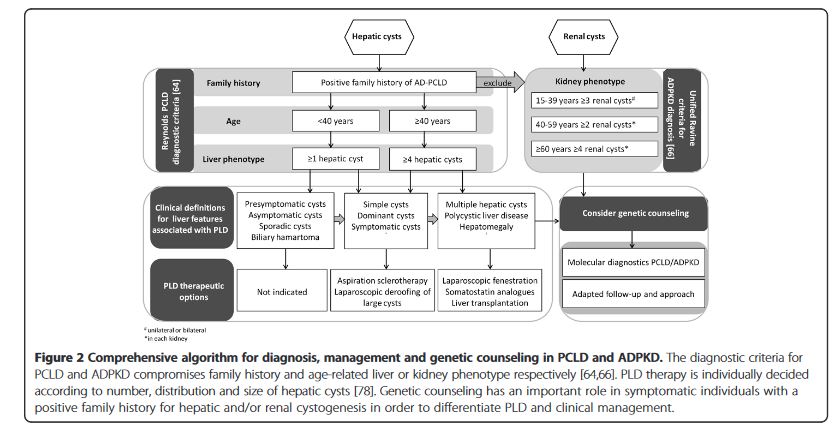
“Polycystic liver disease (PLD) is the result of embryonic ductal plate malformation of the intrahepatic biliary tree.The phenotype consists of numerous cysts spread throughout the liver parenchyma. Cystic bile duct malformations originating from the peripheral biliary tree are called Von Meyenburg complexes (VMC). In these patients embryonic remnants develop into small hepatic cysts and usually remain silent during life. Symptomatic PLD occurs mainly in the context of isolated polycystic liver disease (PCLD) and autosomal dominant polycystic kidney disease (ADPKD).” “Management of adult PLD is based on liver phenotype, severity of clinical features and quality of life. Conservative treatment is recommended for the majority of PLD patients. The primary aim is to halt cyst growth to allow abdominal decompression and ameliorate symptoms. Invasive procedures are required in a selective patient group with advanced PCLD, ADPKD or liver failure. Pharmacological therapy by somatostatin analogues lead to beneficial outcome of PLD in terms of symptom relief and liver volume reduction.”
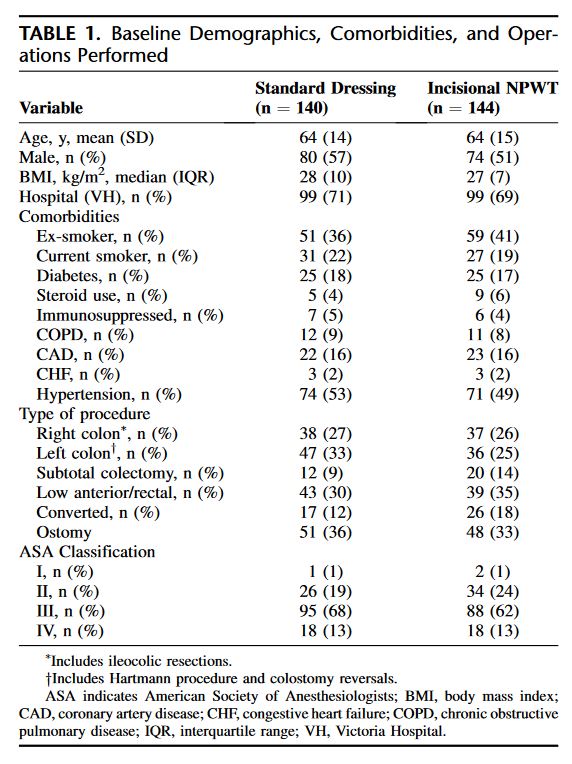
“Surgical site infection (SSI) is one of the most common complications following open colon and rectal surgery. Significant morbidity—secondary to increased length of stay, delay in adjuvant treatments, and psychosocial effects—has been well established in the literature. Further, SSIs confer additional monetary costs to the healthcare system.6 Despite best practice recommendations including prophylactic antibiotics and aseptic technique, SSIs remain common in open colorectal surgery. Rates of SSI in the literature range between 15 and 30%. Increased use of laparoscopy in colorectal surgery has significantly impacted rates of SSI but the uptake of laparoscopy has not been complete as certain patients are not candidates and conversion to open is required in approximately 15% of cases.”
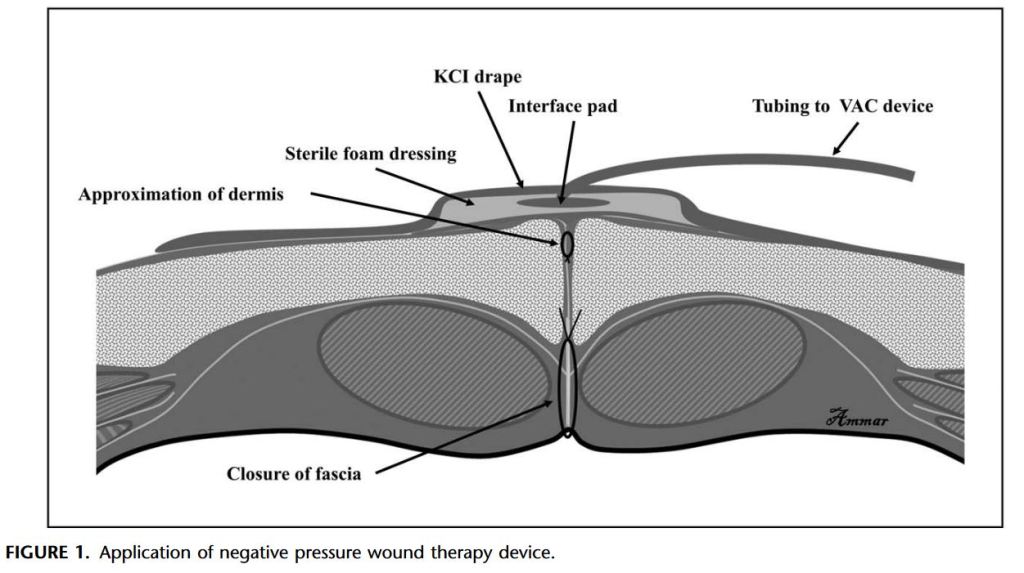
“Despite improvement in infection control, SSIs remain a common cause of morbidity after abdominal surgery. SSI has been associated with an increased risk of reoperation, prolonged hospitalization, readmission, and higher costs. Recent retrospective studies have suggested that the use of negative pressure wound therapy can potentially prevent this complication.”
Surgical site infection (SSI) is a well-characterized morbidity after vascular surgical procedures, especially after infrainguinal and lower extremity bypass. Rates of SSI after these interventions range from 4.8% to 38.5%, which is higher than predicted for “clean” (type I/II) wounds (2%-6%). SSI rates are increased because of the proximity of wounds to the perineum and genitalia, use of prosthetic materials, and disruption of lymphatic vessels during groin incisions; most are attributable to inoculation by skin flora or direct bacterial spread at the time of initial operation.