“Acute severe gastrointestinal bleeding is a common cause of death worldwide. Bleeding can occur from the upper or lower gastrointestinal tract, but upper gastrointestinal bleeding is more common. The leading causes are peptic ulcer, oesophageal varices, and malignancy. The case fatality rate is approximately 10% for upper gastrointestinal bleeding and 3% for lower gastrointestinal bleeding. Many patients re-bleed after initial haemostasis and those that do have a four times increased risk of death. Patients with acute severe gastrointestinal bleeding usually present with haematemesis or melaena. Patients are often haemodynamically unstable and in need of urgent resuscitation. Acute management of gastrointestinal bleeding includes blood product transfusion, medical or endoscopic therapy, and surgery.”
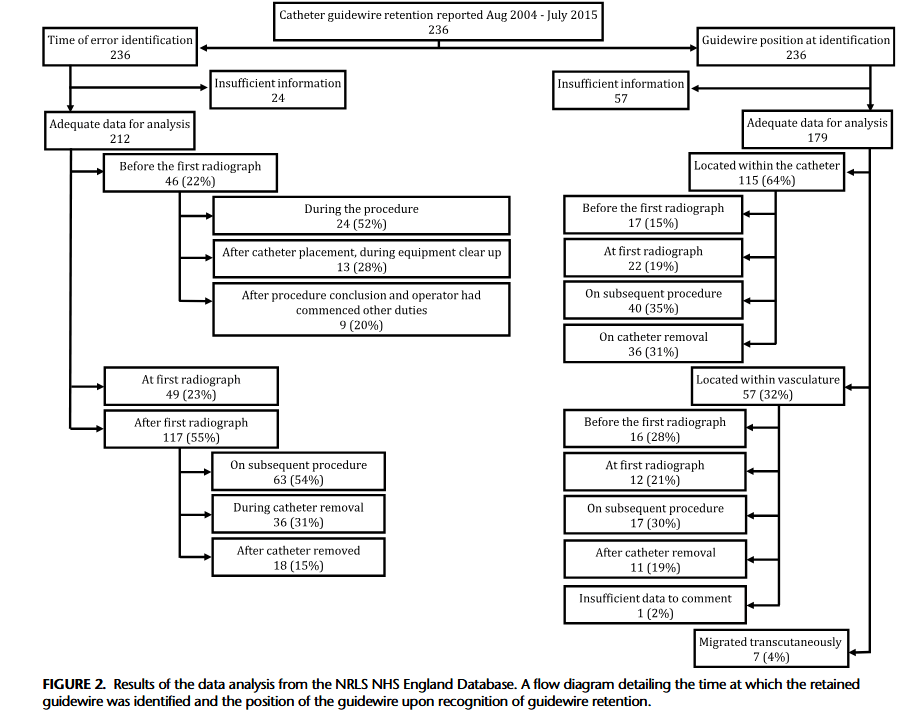
“Central venous catheters (CVC) are commonly used for monitoring and administering medication. The Seldinger technique is routinely used for CVC insertion; however, this technique has an inherent risk of guidewire retention. The mechanism behind guidewire retention is debated, with some authors reporting cases where guidewires “slip” or are sucked into the vasculature at the point of insertion, presumably due to physiological blood flow exhibiting a force on the guidewire that overcomes the frictional force between the guidewire and the CVC lumen, which should prevent guidewire slippage. This is the basis for widely adopted guidance that mandates that operators should hold onto the guidewire at all times while it remains intravascular during CVC insertion. However, this may be an oversimplification of retention events, as most guidewires are likely to remain intraluminally should the operator inadvertently take their hand off them during the procedure. Indeed, the forces exerted by blood flow and pressure differentials are much greater during arterial procedures, although in the opposite direction. If these forces were sufficient to overcome friction, guidewires would be ejected from catheters whenever the operator took his/her hand off the guidewire. When retention occurs, the guidewire can migrate from the catheter into the patient’s vasculature and heart and may cause complications such as arrhythmia, vascular damage, thrombosis, cardiac perforation, and tamponade.”
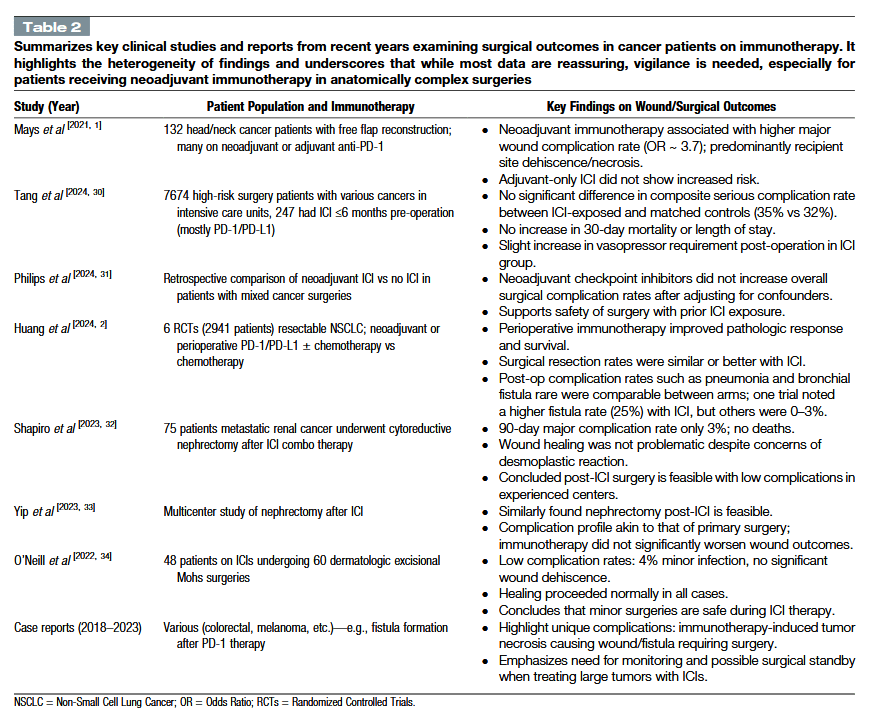
“Wound healing is a complex process requiring a finely tuned immune response. Cancer patients often have risk factors for impaired healing, including older age, malnutrition, steroid use, and prior treatments. Traditionally, oncologic therapies like cytotoxic chemotherapy or anti-angiogenic drugs (e.g., bevacizumab) are known to delay wound healing by suppressing cell proliferation or blood vessel growth. In contrast, immunotherapies stimulate immune activity rather than directly inhibiting regenerative pathways. The net effect of immunotherapy on wound repair is not yet fully understood. Early clinical observations have been mixed—some reports suggest immunotherapy can be given safely during the perioperative period, whereas others have noted higher rates of wound complications in certain settings. Given the increasing overlap of surgery, wound care, and immunotherapy in oncology, a thorough review of current evidence is warranted.”
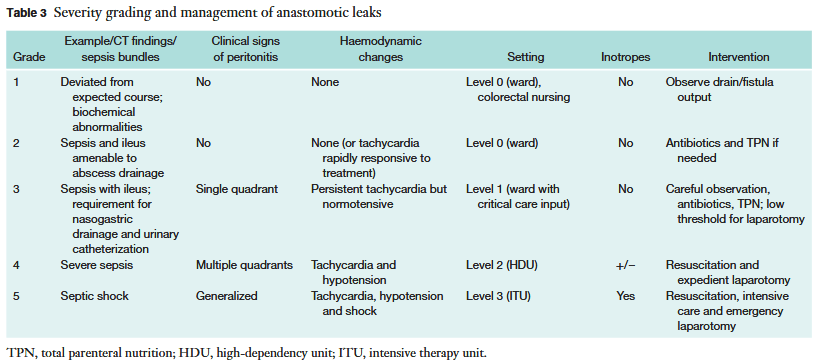
“Anastomotic leak (AL) represents a dreaded complication following colorectal surgery, with a prevalence of 1-19 per cent. There remains a lack of consensus regarding factors that may predispose to AL and the relative risks associated with them. The objective was to perform a systematic review of the literature, focusing on the role of preoperative, intraoperative and postoperative factors in the development of colorectal ALs.”
“In recent years, indocyanine green (ICG) fluorescence imaging has emerged as an alternative tool to enhance the visualization of biliary structures during LC. ICG is a fluorescent dye that, when injected intravenously, is preferentially taken up by the liver and excreted into the bile ducts. When exposed to near-infrared light, ICG causes the biliary structures, such as the CD, CBD, and CA, to fluoresce, making them more distinguishable from surrounding tissues thereby facilitating real-time visualization of biliary structures during the dissection of Calot’s triangle. The timing of ICG injection is critical to ensure that the biliary anatomy lights up distinctly without interference from non-biliary structures. However, the routine use of ICG fluorescence imaging in LC has not yet been standardized, and there is ongoing debate about whether its widespread adoption would significantly reduce the incidence of BDI and improve patient outcomes. This systematic review aims to provide a comprehensive evaluation of the efficacy and safety of ICG fluorescence imaging in LC, specifically comparing its impact on the incidence of BDI to that of conventional white light (WL) imaging.”
Table 4. Comparison of visualization of biliary structures and incidence of BDI using ICG fluorescence vs WL in LC.
BDI, bile duct injury; CBD, common bile duct; CD, cystic duct; CHD, common hepatic duct; ICG, indocyanine green; LC, laparoscopic cholecystectomy; WL, white light; -, not specified
Author(s) and year
Visualization of CD
Visualization of CBD
Visualization of CHD
Visualization of the CD-CBD junction
Incidence of BDI using ICG
Incidence of BDI using WL
Symeonidis et al., 2024
No significant difference (p = 0.225)
No significant difference (p = 0.276)
No significant difference (p = 0.940)
No significant difference (p = 0.827)
0
0
Ma et al., 2023
Before dissecting Calot’s: no significant difference (p = 0.075). After dissecting Calot’s: ICG signifi-cantly improved visualization (p = 0.02)
Before dissecting Calot’s: no significant difference (p = 0.075). After dissecting Calot’s: ICG signifi-cantly improved visualization (p = 0.02)
–
–
0
0
Xu et al., 2023
–
–
–
–
0
0
Stolz et al., 2023
No significant difference
No significant difference
No significant difference
No significant difference
–
–
Lie et al., 2023
Improved RR 1.24, 95% CI 1.07–1.43, p = 0.003
Improved: RR 1.31, 95% CI 1.07–1.60, p = 0.009
–
–
No significant difference: (RR 0.34, 95% CI 0.07–1.58, p = 0.17)
No significant difference: (RR 0.34, 95% CI 0.07–1.58, p = 0.17)
Losurdo et al., 2022
–
–
–
–
0
1.4%, p = 0.728
Lacuzzo et al., 2022
–
–
–
–
0
0
Jin et al., 2022
–
–
–
–
0
1.83%, p = 0.389
Lim et al., 2021
No significant difference: RR = 0.90, p = 0.12, 95% CI 0.79– 1.03, I² = 74%
No significant difference: RR = 0.82, p = 0.09, 95% CI 0.65– 1.03, I² = 87%
ICG significantly improved visualization: RR = 0.58, p = 0.03, 95% CI 0.35–0.93, I² = 91%
No significant difference: RR = 0.68, p = 0.06, 95% CI 0.45– 1.02, I² = 94%
0
2 (0.55%)
Dip et al., 2021
–
–
–
–
1 (0.06%)
12 (0.25%)
Broderick et al., 2021
–
–
–
–
0
1 (0.1%), p = 1
Keeratibharat, 2021
ICG signifi-cantly improved visualization, p = 0.001
ICG signifi-cantly improved visualization, p = 0.002
ICG signifi-cantly improved visualization, p = 0.000
–
0
0
Ambe et al., 2019
–
–
–
–
0
0
Dip et al., 2019
Before dissecting Calot’s: ICG signifi-cantly improved visualization (p ≤ 0.001). After dissecting Calot’s: no significant difference (p = 0.83)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
Before and after dissecting Calot’s: ICG signifi-cantly improved visualization (p < 0.001)
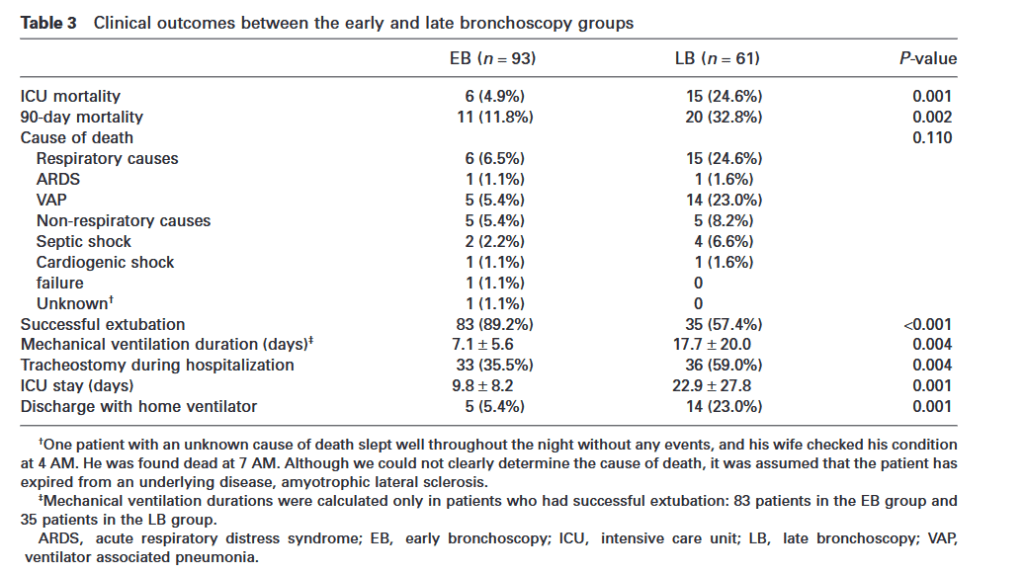
“Aspiration is a process whereby material from the oropharynx and stomach enter the larynx or lower respiratory tract; it is reported to occur in 10.3% of patients who are diagnosed with community-acquired pneumonia and 30% of patients with pneumonia who are admitted from a long-term care facility. Approximately 90% of patients in intensive care units (ICU) also experience aspiration events at least once during their ICU stay. Aspiration pneumonia is an infectious and inflammatory process of microorganisms, which colonize in the aspirated materials. It has been demonstrated that bronchoscopy accompanied with bronchoalveolar lavage (BAL) is helpful for patients with aspiration-induced lung injury in order to reveal causative organisms and determine the appropriate duration of antibiotic treatment. It is also known that the initial administration of appropriate antibiotics can lower the mortality rate in these patients.”
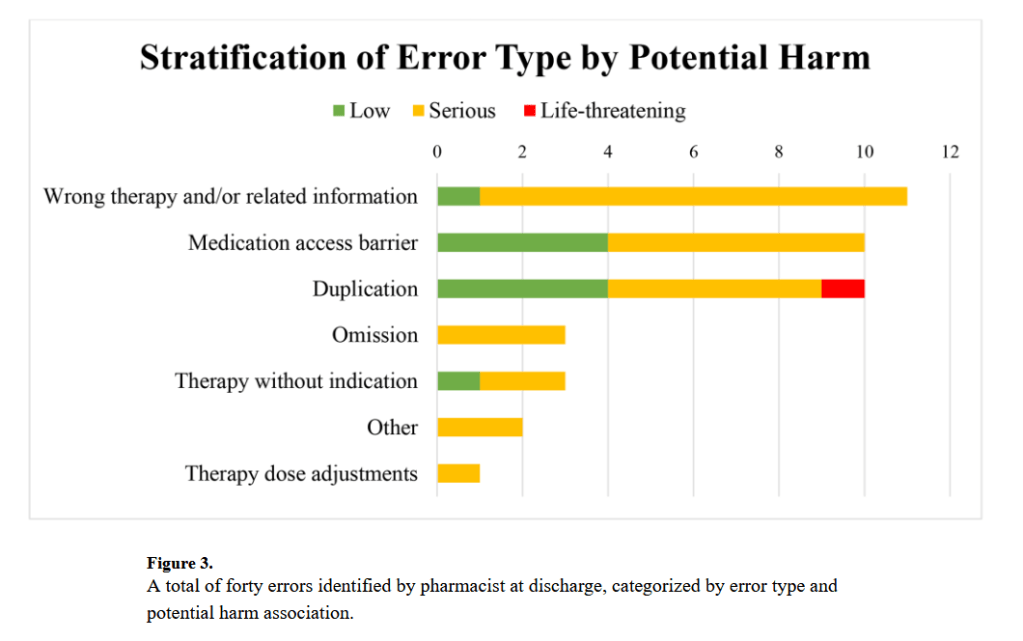
“Medication discrepancies and errors occurring during hospital discharge represent a critical concern, posing significant risks such as adverse patient outcomes, medication-related readmissions, and increased health care costs. Pharmacist-led medication reconciliation at discharge (PMRD) has emerged as a potential solution to enhance medication safety by mitigating medication errors and reducing hospital readmissions. Hospital discharge is a phase of care in which patients often become more vulnerable due to the absence of monitoring and assistance with medication administration. Previous publications from the Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) have revealed a reduction in potentially harmful discrepancies in admission and discharge orders through a multifaceted medication reconciliation implementation model.8,9 However, these studies did not further assess the unintentional discrepancies that were identified, leaving a gap in understanding their potential for patient harm. While Muller and colleagues have evaluated potential patient harm avoided through pharmacist intervention in resolving discharge medication reconciliation discrepancies, there remains a need for further investigation into the financial implications of such interventions.”