Shaffer VO, Owi T, Kumarusamy MA, Sullivan PS, Srinivasan JK, Maithel SK, Staley CA, Sweeney JF, Esper G. Decreasing Hospital Readmission in Ileostomy Patients: Results of Novel Pilot Program. J Am Coll Surg. 2017 Apr;224(4):425-430.
Full-text for Emory users.
BACKGROUND: Nearly 30% of patients with newly formed ileostomies require hospital readmission from severe dehydration or associated complications. This contributes to significant morbidity and rising healthcare costs associated with this procedure. Our aim was to design and pilot a novel program to decrease readmissions in this patient population.
STUDY DESIGN: An agreement was established with Visiting Nurse Health System (VNHS) in March 2015 that incorporated regular home visits with clinical triggers to institute surgeon-supervised corrective measures aimed at preventing patient decompensation associated with hospital readmissions. Thirty-day readmission data for patients managed with and without VNHS support for 10.5 months before and after implementation of this new program were collected.
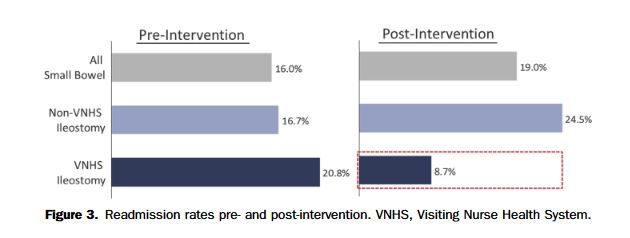
RESULTS: Of 833 patients with small bowel procedures, 162 were ileostomies with 47 in the VNHS and 115 in the non-VNHS group. Before program implementation, VNHS (n = 24) and non-VNHS patients (n = 54) had similar readmission rates (20.8% vs 16.7%). After implementation, VNHS patients (n = 23) had a 58% reduction in hospital readmission (8.7%) and non-VNHS patient hospital readmissions (n = 61) increased slightly (24.5%). Total cost of readmissions per patient in the cohort decreased by >80% in the pilot VNHS group.
CONCLUSIONS: Implementation of a novel program reduced the 30-day readmission rate by 58% and cost of readmissions per patient by >80% in a high risk for readmission patient population with newly created ileostomies. Future efforts will expand this program to a greater number of patients, both institutionally and systemically, to reduce the readmission-rate and healthcare costs for this high-risk patient population.