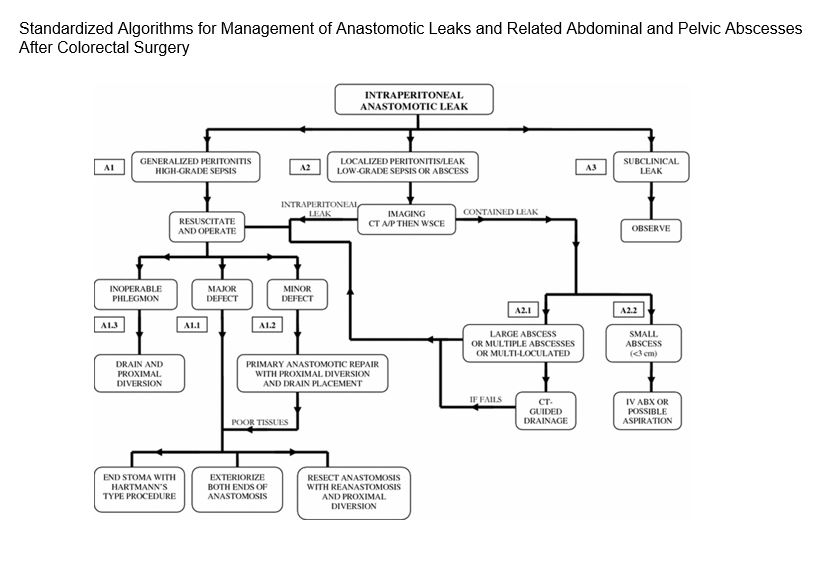
“The risk factors and incidence of anastomotic leak following colorectal surgery are well reported in the literature. However, the management of the multiple clinical scenarios that may be encountered has not been standardized.” In this study, “management scenarios were divided into those for intraperitoneal anastomoses, extraperitoneal (low pelvic) anastomoses, and anastomoses with proximal diverting stomas. Management options were then based on the clinical presentation and radiographic findings and organized into three interconnected algorithms.”
Recommendations for the management of intraperitoneal anastomotic leak with references to the pertinent sections of this article for more information. KEY: IV ABX=intravenous antibiotics; CT=computed tomographic; WSCE=water soluble contrast enema; CT A/P=computed tomographic scan of the abdomen and pelvisContinue reading →
“Acute mesenteric ischemia (AMI) accounts for approximately 1:1000 acute hospital admissions in the United States, and the incidence is on the rise likely due to an aging population as well as the prolonged survival of critically ill patients. AMI can be caused by a reduction in blood flow from arterial occlusion, venous occlusion, arterial vasospasm, or a low-flow state. Regardless of the etiology of the disease, rapid diagnosis and treatment of AMI is of critical importance”
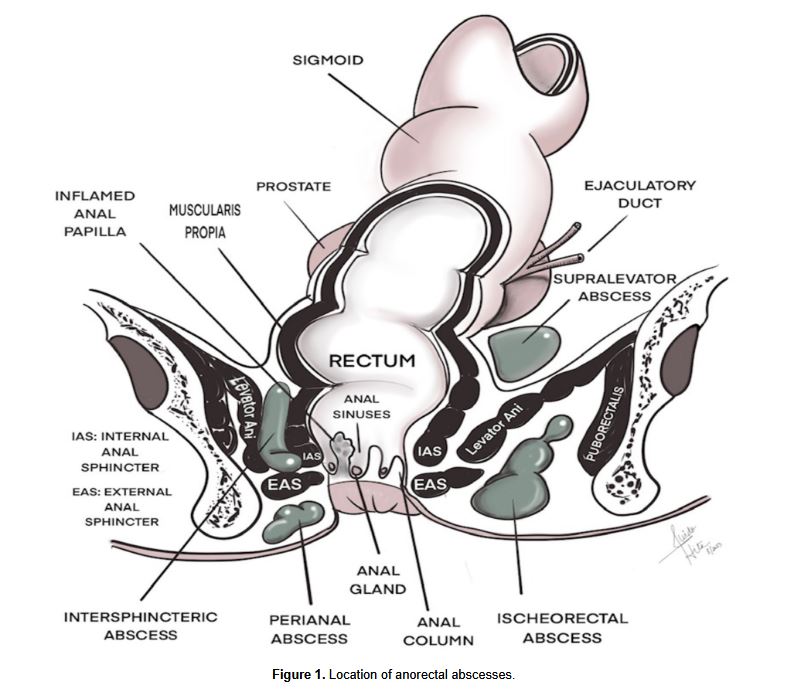
“Anorectal infections in neutropenic leukemia patients are a significant and potentially life-threatening complication. The pathogenesis of this condition is not entirely understood and believed to be multifactorial, including mucosal injury as a result of cytotoxic drugs, profound neutropenia and impaired host defense. Establishing an early diagnosis is key and often made clinically on the basis of signs and symptoms, but also from imaging studies demonstrating perianal inflammation or fluid collection. The management of anorectal infections in neutropenic leukemia patients is not straightforward, as there are no well-conducted studies on this entity.”
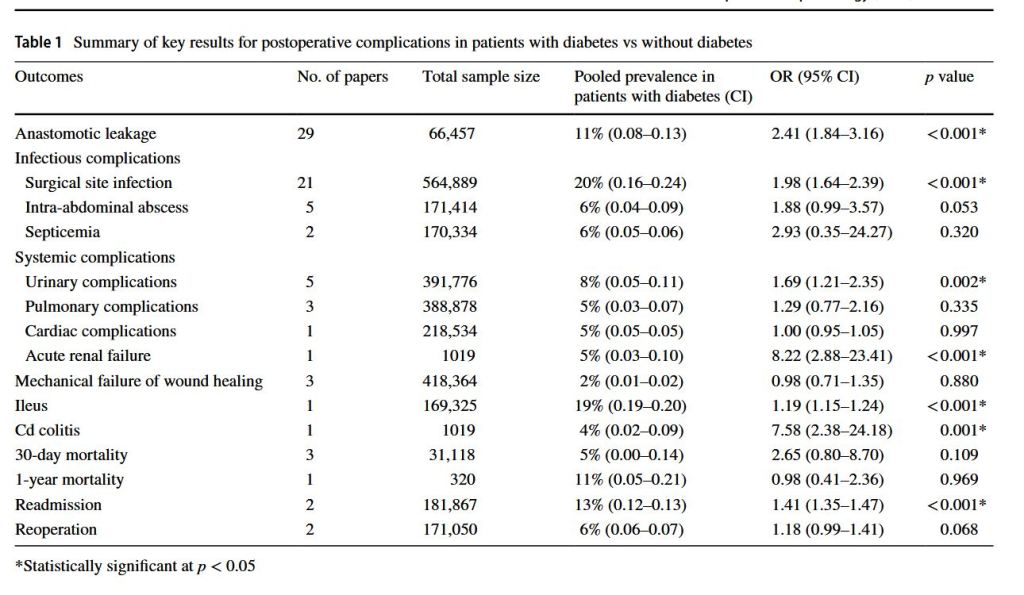
“Diabetes continues to be a significant comorbidity that needs to be accounted for during surgical planning. Furthermore, undiagnosed diabetes or ‘pre-diabetes’ results in an underestimation of the true number of patients with diabetes having colorectal surgery, with studies reporting that the true prevalence of diabetes in hospitalised patients has been understated by up to 40%. In the existing literature, poor glycemic control and hyperglycemia has been associated with impaired wound healing and increased susceptibility to infections,leading to an elevated risk of postoperative complications.”
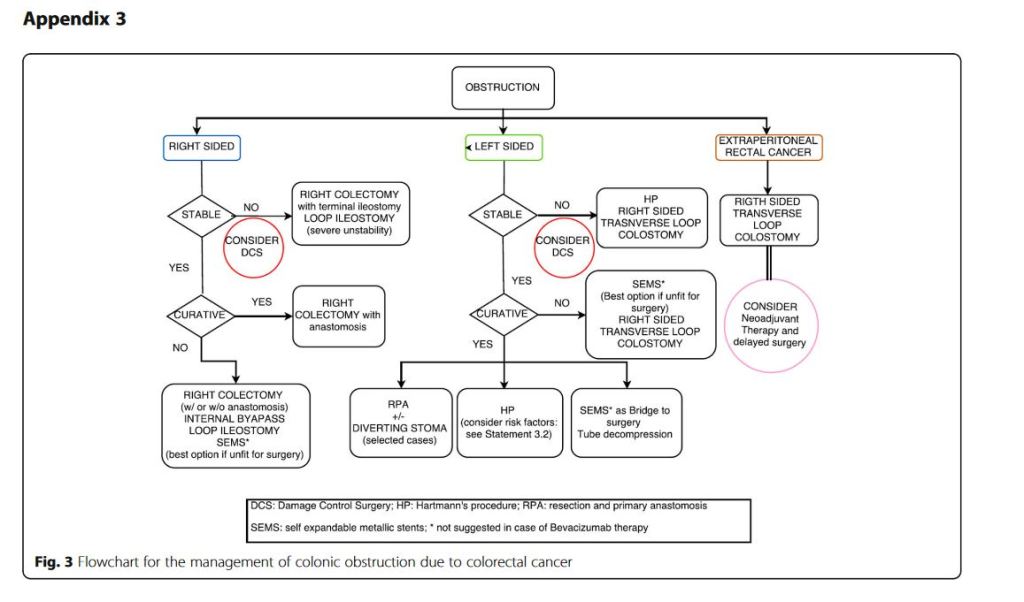
“Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).” “CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann’s procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted. With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.”
“Conclusions: grey areas and opportunities for improvements
We found some limitations within the present guidelines:
– They fail to cover all the possible abdominal scenarios when colon cancer occurs as an emergency: for example, associated resections were not taken into considerations, neither we discussed about therapeutic strategies in case of evidence of peritoneal carcinomatosis. – Despite our attempts to underline suggestions in case of low technical resources, the present guidelines are generally oriented toward hospitals with high level of resources.
On the other side, in our opinion, the current guidelines suggest some stimuli for doctors involved in this field:
– To review the approach to patient suffering from abdominal pain by introducing and promoting the use of bedside abdominal US. – To bear in mind that the emergency surgeon should have a strong oncologic background or that the specialised colorectal surgeon should have a strong background of surgical pathophysiology, emergency surgery and damage control philosophy. – To promote the use of clinical pathways within singular Hospitals”
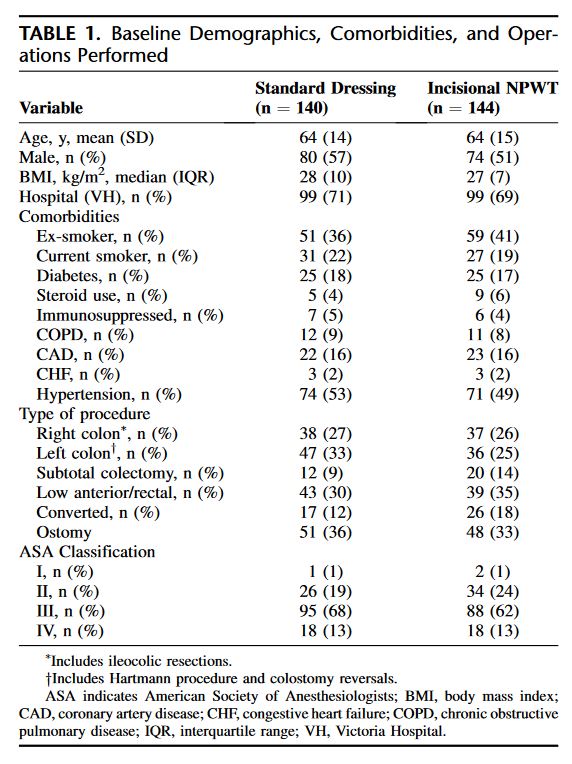
“Surgical site infection (SSI) is one of the most common complications following open colon and rectal surgery. Significant morbidity—secondary to increased length of stay, delay in adjuvant treatments, and psychosocial effects—has been well established in the literature. Further, SSIs confer additional monetary costs to the healthcare system.6 Despite best practice recommendations including prophylactic antibiotics and aseptic technique, SSIs remain common in open colorectal surgery. Rates of SSI in the literature range between 15 and 30%. Increased use of laparoscopy in colorectal surgery has significantly impacted rates of SSI but the uptake of laparoscopy has not been complete as certain patients are not candidates and conversion to open is required in approximately 15% of cases.”