Burch JM, Cox CL, Feliciano DV, Richardson RJ, Martin RR. Management of the difficult duodenal stump. Am J Surg. 1991 Dec;162(6):522-6.
Full-text for Emory users.
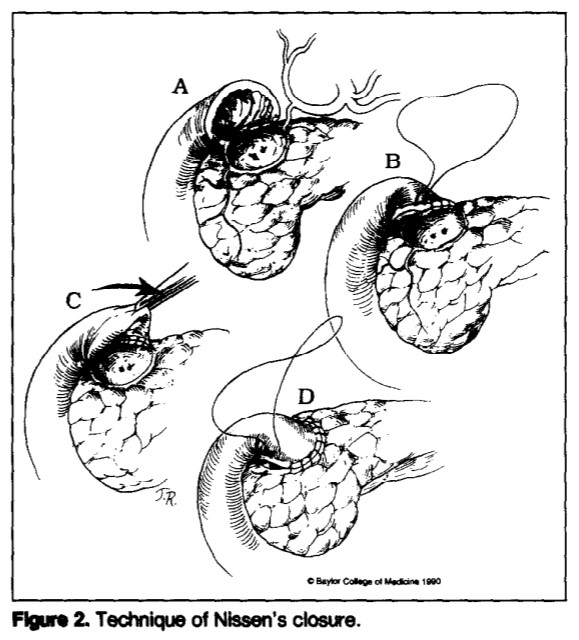
Abstract: Leakage from the duodenal stump has been the most feared complication of the Billroth II reconstruction following gastric resection. The purpose of our study was to evaluate four methods of duodenal stump closure in 200 patients. One hundred and forty-seven (74%) patients had duodenal ulcers; 28 (14%) had gastric ulcers; and 25 (13%) had a variety of other inflammatory conditions. The most common indication for operation was acute hemorrhage (51%), followed by perforation (24%), intractability (15%), and obstruction (10%). Conventional duodenal closures were performed in 160 (80%) patients, Nissen’s closure in 25 (13%), Bancroft’s closure in 6 (3%), and tube duodenostomy in 9 (5%). Duodenal leaks occurred in four (2.5%) patients with conventional closures and in three (33%) patients with tube duodenostomies. No leaks occurred in patients with Nissen’s or Bancroft’s closures. The hospital mortality rate for the series was 9.5%; however, no patient who developed a duodenal leak died. We conclude that Nissen’s and Bancroft’s closures were safe and effective, but that tube duodenostomy did not reliably prevent uncontrolled leakage.