“Operative internal drainage has been standard treatment for chronic unresolved pancreatic pseudocysts (PPs). Recently, percutaneous external drainage (PED) has become the primary mode of treatment at many medical centers.”
“ Operative management for PPs appears to be superior to CT-guided PED. Although the later was often successful, it required major salvage procedures in one third of the patients. An expectant management protocol may be suitable for selected patients.”
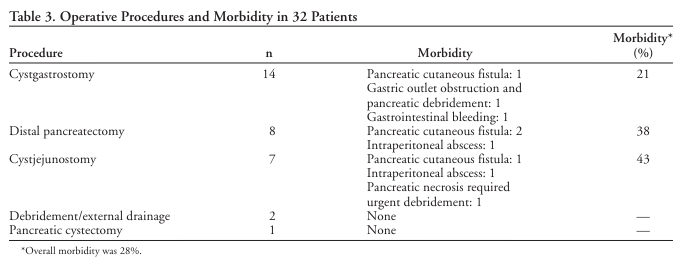
“Pancreatic necrosis is the most devastating complication of acute pancreatitis. Management of this complex disease has improved dramatically over the past decade, and mortality rates are regularly reported in the range of 20% instead of the 50% to 70% range reported in the 1970s. Despite this improvement, 80% of deaths from acute pancreatitis evolve from infectious complications of pancreatic and peripancreatic necrosis.”
“Chronic pancreatitis (CP) is a progressive fibro-inflammatory disease of the pancreas leading to irreversible parenchymal damage with gradual loss of exocrine and endocrine functions. The most common and debilitating manifestation of this disease is intractable pain which may lead to loss of work, unemployment, narcotic dependence, and impairment of the quality of life (QOL). About 30–50% of patients with CP will require surgery during their life time.2,3 Several surgical procedures have been described in the literature, and these are broadly classified as drainage, resectional or a combination of the two. Each respective procedure is chosen based on the degree of pancreatic ductal dilatation, glandular morphology, local complications, and to some extent on the experience and preference of the surgeon. The Frey procedure (FP) has emerged over the past 30 years as one of the most commonly performed operations for painful CP associated with enlarged pancreatic head. The procedure results in substantial and sustained pain relief in the majority of patients. Like other major operations, FP also is associated with several post operative complications.”
“Patients with extrahepatic portal vein thrombosis may present from infancy through adulthood with variceal bleeding. Physiologically, such patients differ from patient s with cirrhosis and variceal bleeding in that they have a normal liver and maintain good portal perfusion through hepatopedal collaterals.” “Therapeutic options range from noninterventive, through ablative procedures, to shunt operations. The goal should be definitive control of bleeding and return to a normal lifestyle. Distal splenorenal shunt offers the best option if technically feasible, but if no shuntable veins are patent, ablative procedures and sclerotherapy may be required. A noninterventive, noninvestigational approach is inappropriate in patients who can be offered definitive therapy. Splenectomy for hypersplenism should not be done in these patients.” (Galloway)
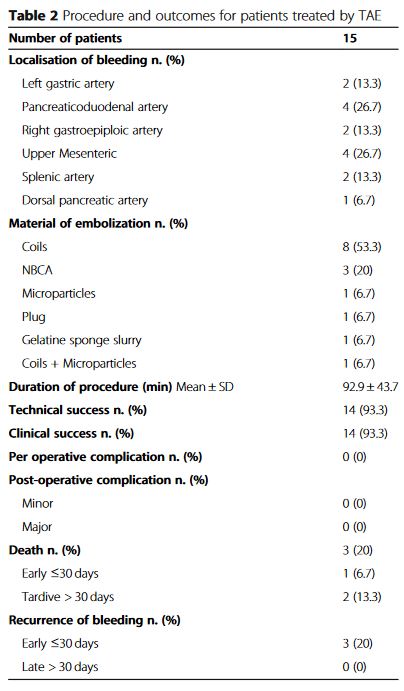
“Mesenteric bleeding (MB) occurs rarely and its frequency is not well known. It corresponds to bleeding from mesenteric vessels in the abdominal cavity, without intra-luminal digestive bleeding. Although relatively rare, this pathology can be life-threatening if left undiagnosed and untreated. Clinically, MB are characterized by non-systematised abdominal pain and sudden blood loss. MB has many causes such as a post operative complication (especially after pancreaticoduodenectomy), traumatism, tumour, or may be idiopathic with no cause found. CT-scan is the gold standard of diagnostic imaging to identify the cause of MB. While the management of upper and lower gastrointestinal bleeding has been well established, the management of active mesenteric bleeding is less defined in the medical literature.”
“Pancreas-sparing duodenectomy, although technically demanding, eliminates the need for pancreatic resection. Pancreas-sparing duodenectomy is associated with good absorptive capacity, weight gain, and quality of life. Furthermore, it may reduce the risk of subsequent malignancy. Long-term surveillance, however, is still required. Pancreas-sparing duodenectomy is contraindicated in the setting of malignancy.”
“Pulmonary complications remain relatively high in morbidities that arise after liver surgery and are associated with increased length of hospital stay and higher cost. Identification of possible risk factors in this retrospective analysis may help reduce operative morbidity and achieve better outcomes.”