
Vashist YK, et al. Management of the difficult duodenal stump in penetrating duodenal ulcer disease: a comparative analysis of duodenojejunostomy with “classical” stump closure (Nissen-Bsteh). Langenbecks Arch Surg. 2012 Dec;397(8):1243-9.
Full-text for Emory users.
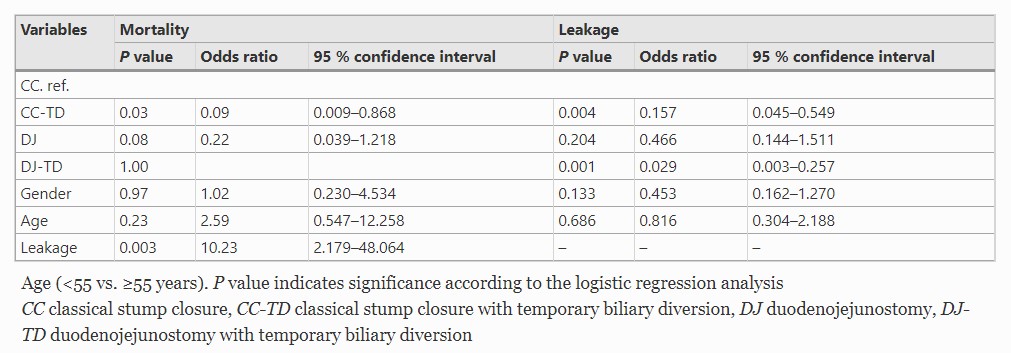
Table 4. Multivariable Analysis for Perioperative Mortality and Leakage in All 124 Patients
Background: Duodenal stump insufficiency after surgery for penetrating gastroduodenal ulcer is associated with substantial mortality. “Classical” technique of closing a difficult duodenal stump (Nissen-Bsteh) has, up to now, not been compared with duodenojejunostomy (DJ) in larger patient sets. This also refers to the potential benefit of a gastric and biliary diversion under such conditions. The aim of the present study was to compare classical duodenal closure (CC) with DJ and to evaluate the impact of gastric and biliary diversion on postoperative outcome after surgery for penetrating, high-risk duodenal ulcer in a matched control study.
