Gupta V, Jain G. Safe laparoscopic cholecystectomy: Adoption of universal culture of safety in cholecystectomy. World J Gastrointest Surg. 2019 Feb 27;11(2):62-84.
Critical View of Safety in laparoscopic cholecystectomy
Reply

Gupta V, Jain G. Safe laparoscopic cholecystectomy: Adoption of universal culture of safety in cholecystectomy. World J Gastrointest Surg. 2019 Feb 27;11(2):62-84.
Tapson VF, Friedman O. Systemic Thrombolysis for Pulmonary Embolism: Who and How. Tech Vasc Interv Radiol. 2017 Sep;20(3):162-174.
Full-text for Emory users.
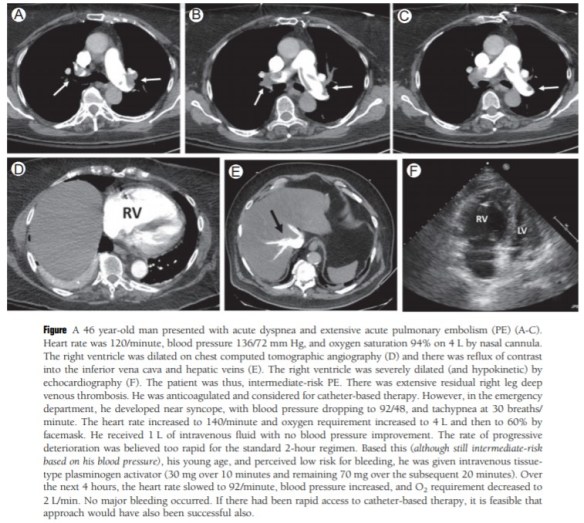
“For several decades, clinicians and clinical trialists have worked toward a more aggressive, yet safe solution for patients with intermediate-risk PE. Standard-dose thrombolysis, low-dose systemic thrombolysis, and catheter-based therapy which includes a number of devices and techniques, with or without low-dose thrombolytic therapy, have offered potential solutions and this area has continued to evolve. On the basis of heterogeneity within the category of intermediate-risk as well as within the high-risk group of patients, we will focus on the use of systemic thrombolysis in carefully selected high- and intermediate-risk patients. In certain circumstances when the need for aggressive therapy is urgent and the bleeding risk is acceptable, this is an appropriate approach, and often the best one.”
More PubMed results on systemic thrombolysis.
Christopherson R, Beattie C, Frank SM, Norris EJ, Meinert CL, Gottlieb SO, Yates H, Rock P, Parker SD, Perler BA, et al. Perioperative morbidity in patients randomized to epidural or general anesthesia for lower extremity vascular surgery. Anesthesiology. 1993 Sep;79(3): 422-34.
Full-text for Emory users.
Background: Perioperative morbidity may be modifiable in high risk patients by the anesthesiologist’s choice of either regional or general anesthesia. This clinical trial compared outcomes between epidural (EA) and general (GA) anesthesia/analgesia regimens in a group of patients at high risk for cardiac and other morbidity who were undergoing similarly stressful surgical procedures.
Oberkofler CE, et al. A multicenter randomized clinical trial of primary anastomosis or Hartmann’s procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann Surg. 2012 Nov; 256(5):819-26; discussion 826-7.
Full-text for Emory users.
Results: Patient demographics were equally distributed in both groups (Hinchey III: 76% vs 75% and Hinchey IV: 24% vs 25%, for HP vs PA, respectively). The overall complication rate for both resection and stoma reversal operations was comparable (80% vs 84%, P = 0.813). Although the outcome after the initial colon resection did not show any significant differences (mortality 13% vs 9% and morbidity 67% vs 75% in HP vs PA), the stoma reversal rate after PA with diverting ileostomy was higher (90% vs 57%, P = 0.005) and serious complications (Grades IIIb-IV: 0% vs 20%, P = 0.046), operating time (73 minutes vs 183 minutes, P < 0.001), hospital stay (6 days vs 9 days, P = 0.016), and lower in-hospital costs (US $16,717 vs US $24,014) were significantly reduced in the PA group.
Conclusions: This is the first randomized clinical trial favoring PA with diverting ileostomy over HP in patients with perforated diverticulitis.
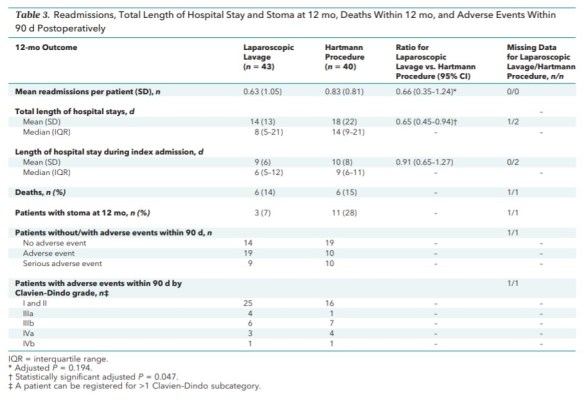
Thornell A, et al. Laparoscopic Lavage for Perforated Diverticulitis With Purulent Peritonitis: A Randomized Trial. Ann Intern Med. 2016 Feb 2;164(3):137-45.
Full-text for Emory users.
Wu Z, Zhou J, Pankaj P, Peng B. Comparative treatment and literature review for laparoscopic splenectomy alone versus preoperative splenic artery embolization splenectomy. Surg Endosc. 2012 Oct;26(10):2758-66.
Full-text for Emory users.
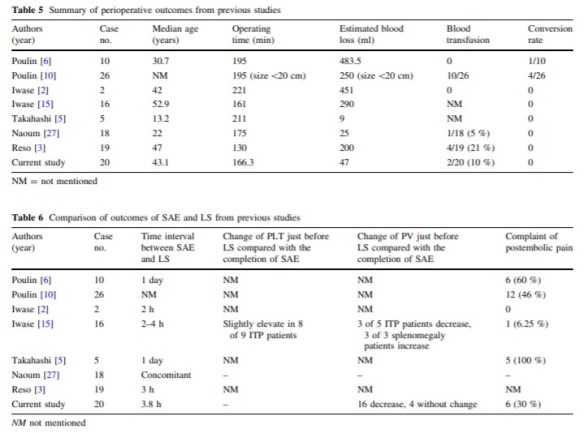
Results: Preoperative splenic artery embolization plus laparoscopic splenectomy was successfully performed in all patients in group 1. One patient in group 2 required an intraoperative conversion to traditional open splenectomy because of severe blood loss. Compared with group 2, significantly shorter operating time, less intraoperative blood loss, and shorter postoperative hospital stay were noted in group 1. No marked significant differences in postoperative complications of either group were observed. Compared with group 3, group 1 had less intraoperative blood loss, shorter postoperative stay, and fewer complications. No significant differences were found in operating time. There was a marked increase in platelet count and white blood count in both groups during the follow-up period.
Conclusions: Preoperative splenic artery embolization with laparoscopic splenectomy reduced the operating time and decreased intraoperative blood loss when compared with laparoscopic splenectomy alone or open splenectomy. Splenic artery embolization is a useful intraoperative adjunctive procedure for patients with splenomegaly because of the benefit of perioperative outcomes.
Seymour MT, Morton D. FOxTROT: an international randomised controlled trial in 1052 patients (pts) evaluating neoadjuvant chemotherapy (NAC) for colon cancer. J Clin Oncol. 2019 May;37(15 Suppl):3504-3504.
Conclusions: NAC was well tolerated and safe, with no increase in perioperative morbidity and a trend toward fewer serious postoperative complications. Evidence of histological regression was seen in 59% pts after NAC, including some pCRs. This resulted in marked histological downstaging and a halving of the rate of incomplete resections. We observed an improvement in 2-yr failure rate (HR=0.77), but this fell short of statistical significance (p=0.11). NAC for colon cancer improves surgical outcomes and can now be considered as a treatment option; longer follow-up and further trials are required to confirm the long-term benefits, refine its use and optimise case selection. ClinicalTrials.gov Identifier: NCT00647530
Foxtrot Collaborative Group. Feasibility of preoperative chemotherapy for locally advanced, operable colon cancer: the pilot phase of a randomised controlled trial. Lancet Oncol. 2012 Nov;13(11):1152-60.
The FOxTrOT website (University of Birmingham)
Maxwell DW, Jajja MR, Ferez-Pinzon A, Pouch SM, Cardona K, Kooby DA, Maithel SK, Russell MC, Sarmiento JM. Bile cultures are poor predictors of antibiotic resistance in postoperative infections following pancreaticoduodenectomy.HPB (Oxford). 2019 Oct 26:S1365-182X(19)30756-7.
Results: Common patient characteristics of 522 included patients were 65-years-old, Caucasian (75.5%), male (54.2%), malignant indication (79.3%), and preoperative biliary stent (59.0%). Overall, 275 (89.6%) BCs matured identifiable isolates with 152 (55.2%) demonstrating polymicrobial growth. Ninety-two (17.6%) SOICs were obtained: 48 and 44 occurred in patients with and without intraoperative BCs. Stents were associated with bacteriobilia (85.7%, K = 0.947, p < 0.001; OR 22.727, p < 0.001), but not postoperative infections (15.2%; K = 0.302, p < 0.001; OR 1.428, p = 0.122). Forty-eight patients demonstrated paired BC/SOICs to evaluate. Pathogenic concordance of this group was 31.1% (K = 0.605, p < 0.001) while SRP concordance of matched pathogens was 46.7% (K = 0.167, p = 0.008).
Conclusion: Bile cultures demonstrate poor concordance with the susceptibility/resistance patterns of postoperative infections following pancreaticoduodenectomy and may lead to inappropriate antibiotic therapies.

